

Role of Preoperative Embolization in Surgical Management of Carotid Body Tumors: A Systematic Review and Meta-Analysis
Abstract
Introduction
Methods
Eligibility Criteria
Information Sources
Search Strategy and Selection Process
Data Extraction and Outcomes
Data Preparation Measures
Risk of Bias Assessment
Data Synthesis and Analysis
Results
Study Selection

Study and Patient Characteristics
| Author and year | Study design | Patient enrollment period | Country | Total patients in EMB | Total patients in NEMB | Follow-up period (months) |
|---|---|---|---|---|---|---|
| Amato et al., 201914 | RT | 2004–2016 | Italy | 10 | 23 | 26–48 |
| Avgerinos et al., 201115 | R | 1975–2009 | Greece | 4 | 23 | 6–288 |
| Bercin et al., 201516 | R | 2010–2014 | Turkey | 7 | 6 | - |
| Cobb et al., 201817 | R | 2006–2013 | USA | 75 | 453 | - |
| del Guercio et al., 201318 | R | 1972–2012 | Italy | 5 | 20 | 9–216 |
| Gözen et al., 202019 | R | 2012–2019 | Turkey | 15 | 11 | - |
| Gwon et al., 201120 | R | 1998–2008 | South Korea | 14 | 2 | - |
| Ikeda et al., 201821 | R | 1995–2015 | Japan | 76 | 18 | - |
| Law et al., 201722 | R | 1994–2014 | China | 9 | 11 | 94 |
| Li et al., 201023 | R | 1997–2007 | China | 33 | 29 | 13–96 |
| Li et al., 202224 | R | 2007–2020 | China | 130 | 39 | 2–156 |
| Lim et al., 201025 | R | - | South Korea | 7 | 6 | 15–64 |
| Liu et al., 201826 | R | 2002–2016 | China | 31 | 27 | - |
| Mohebali et al., 202027 | R | 1996–2018 | USA | 27 | 41 | - |
| Mourad et al., 201628 | R | 1997–2014 | USA | 53 | 43 | 3–84 |
| Osofsky et al., 202129 | R | 2001–2019 | USA | 20 | 28 | - |
| Power et al., 201230 | R | 1985–2010 | USA | 29 | 69 | 0–236 |
| Rao et al., 201731 | R | 2010–2015 | India | 1 | 6 | 12 |
| Sen et al., 201332 | R | 2005–2011 | India | 15 | 19 | 1–60 |
| Wernick et al., 202033 | R | 2002–2019 | USA | 9 | 16 | - |
| Wu et al., 202234 | R | 2003–2019 | China | 28 | 28 | 1–48 |
| Yazman et al., 202235 | R | 2005–2020 | Turkey | 23 | 27 | 3–90 |
| Zeitler et al., 201036 | R | 1989–2009 | USA | 10 | 15 | - |
| Zhang et al., 201237 | R | 2005–2010 | China | 21 | 8 | 12–48 |
| Zhang et al., 201838 | R | 2006–2016 | China | 11 | 18 | 12–156 |
| Author and year | Embolic agent used | Time from embolization to surgery (hrs) |
|---|---|---|
| Amato et al., 201914 | PVA | - |
| Avgerinos et al., 201115 | PVA | 48 |
| Bercin et al., 201516 | PVA | 24–48 |
| Cobb et al., 201817 | - | 0–72 |
| del Guercio et al., 201318 | - | 24 |
| Gözen et al., 202019 | PVA | 24–48 |
| Gwon et al., 201120 | PVA and gelfoam | 48–72 |
| Ikeda et al., 201821 | - | 24–48 |
| Law et al., 201722 | - | - |
| Li et al., 201023 | PVA, gelfoam, and microcoils | 24–144 |
| Li et al., 202224 | PVA and microspheres | 24 |
| Lim et al., 201025 | PVA | 48 |
| Liu et al., 201826 | - | 24–48 |
| Mohebali et al., 202027 | - | - |
| Mourad et al., 201628 | - | 0–48 |
| Osofsky et al., 202129 | PVA | 24 |
| Power et al., 201230 | PVA | 24–72 |
| Rao et al., 201731 | EVOH | - |
| Sen et al., 201332 | PVA and gelfoam | 0–24 |
| Wernick et al., 202033 | - | - |
| Wu et al., 202234 | Microcoils | 24–72 |
| Yazman et al., 202235 | PVA | 24–48 |
| Zeitler et al., 201036 | PVA | 48–72 |
| Zhang et al., 201237 | PVA and fibered platinum coils | 0–48 |
| Zhang et al., 201838 | PVA, tornado microcoil, and EVOH | 0–48 |
| Author and year | Patient group | Total patients (n) | Male:female (n) | Mean age (SD) | Mean tumor size in cm (SD) | Shamblin classification (I/II/III) |
|---|---|---|---|---|---|---|
| Amato et al., 201914 | EMB | 10 | 3:7 | 59 | 4.7 | 0/7/4 |
| NEMB | 23 | 11:12 | 4.1 | 0/16/7 | ||
| Avgerinos et al., 201115 | EMB | 4 | 13:14 | 46 | - | 0/2/2 |
| NEMB | 23 | - | 8/9/8 | |||
| Bercin et al., 201516 | EMB | 7 | 2:5 | 47.4 | 4.6 | 0/6/1 |
| NEMB | 6 | 1:5 | 49.8 | 4.16 | 0/6/0 | |
| Cobb et al., 201817 | EMB | 75 | 24:51 | 50.6 (15.9) | - | - |
| NEMB | 453 | 146:299 | 55.4 (15.4) | - | - | |
| del Guercio et al., 201318 | EMB | 5 | 18:7 | 39.7 (13.5) | - | - |
| NEMB | 20 | - | - | |||
| Gözen et al., 202019 | EMB | 15 | 5:10 | 41.53 (11.03) | 3.9 (1.19) | 1/7/7 |
| NEMB | 11 | 3:8 | 48.18 (14.39) | 3.09 (1.38) | 3/7/1 | |
| Gwon et al., 201120 | EMB | 14 | 5:11 | 41.7 | 3.34 (1.24) | 8/4/5 |
| NEMB | 2 | |||||
| Ikeda et al., 201821 | EMB | 76 | 63:87 | 47.6 (13.3) | 3.45 | 19/48/9 |
| NEMB | 18 | 4/11/3 | ||||
| Law et al., 201722 | EMB | 9 | 4:16 | 37 (9.9) | 3.8 (1.5) | - |
| NEMB | 11 | 3.9 (1.6) | - | |||
| Li et al., 201023 | EMB | 33 | 15:18 | 40.2 | - | 0/11/25 |
| NEMB | 29 | 12:17 | 44.3 | - | 0/9/21 | |
| Li et al., 202224 | EMB | 130 | 85:84 | 37.24 (12.02) | 4.35 (1.5) | 5/105/20 |
| NEMB | 39 | 3.54 (1.6) | 7/27/5 | |||
| Lim et al., 201025 | EMB | 7 | 6:7 | 45.3 (8.1) | 3.5 | 0/4/3 |
| NEMB | 6 | 3.9 | 1/0/5 | |||
| Liu et al., 201826 | EMB | 31 | 6:25 | 43.52 (10.38) | 5.16 (1.57) | 0/22/9 |
| NEMB | 27 | 8:19 | 42.78 (9.08) | 5.09 (1.57) | 0/18/9 | |
| Mohebali et al., 202027 | EMB | 27 | 27:41 | 50.83 | - | - |
| NEMB | 41 | - | - | |||
| Mourad et al., 201628 | EMB | 53 | 50:46 | 49.2 | - | 13/24/16 |
| NEMB | 43 | - | 10/26/12 | |||
| Osofsky et al., 202129 | EMB | 20 | 3:17 | 47 (16) | 4 (0.7) | 1(I)/18 (II & III) |
| NEMB | 28 | 5:23 | 52 (14) | 3.3 (1) | 6(I)/22 (II & III) | |
| Power et al., 201230 | EMB | 29 | 8:21 | 47 | 4.7 | 0/21/12 |
| NEMB | 69 | 32:37 | 48 | 4.1 | 0/50/21 | |
| Rao et al., 201731 | EMB | 1 | - | - | - | 0/1/0 |
| NEMB | 6 | - | - | - | 3/3/0 | |
| Sen et al., 201332 | EMB | 15 | 21:13 | 38.2 | - | 0/2/13 |
| NEMB | 19 | - | 1/4/14 | |||
| Wernick et al., 202033 | EMB | 9 | 9:16 | 49 | 4 | 4/10/11 |
| NEMB | 16 | 3 | ||||
| Wu et al., 202234 | EMB | 28 | 8:20 | 46.6 | 4.8 | 2/13/13 |
| NEMB | 28 | 8:20 | 42.6 | 4.6 | 2/14/12 | |
| Yazman et al., 202235 | EMB | 23 | 4:19 | 49 (3.05) | 4.3 (0.3) | 4/9/10 |
| NEMB | 27 | 5:22 | 51.7 (3.2) | 3.5 (0.2) | 8/15/5 | |
| Zeitler et al., 201036 | EMB | 10 | 4:6 | 41 | 4.8 | - |
| NEMB | 15 | 6:9 | 43.7 | 4.4 | - | |
| Zhang et al., 201237 | EMB | 21 | 22:10 | 47 | 4.5 | 2/14/5 |
| NEMB | 8 | 3.9 | 1/5/2 | |||
| Zhang et al., 201838 | EMB | 11 | 4:7 | 47 | 6 | 1/7/3 |
| NEMB | 18 | 7:11 | 45 | 4.5 | 7/9/2 |
Outcomes
| Author and year | Patient group | Mean operative time in min (SD) | Mean intraoperative blood loss in mL (SD) | Mean post-op hospital stay, days (SD) | TIA/stroke (n) | Vascular injury (n) | Cranial nerve injury(n) |
|---|---|---|---|---|---|---|---|
| Amato et al., 201914 | EMB | 250 | 263 | 4.1 | - | 5 | 7 |
| NEMB | 265 | 599 | 4.2 | - | 21 | 11 | |
| Avgerinos et al., 201115 | EMB | - | 415 (182.6) | - | - | - | - |
| NEMB | - | 710 (350) | - | - | - | - | |
| Bercin et al., 201516 | EMB | 172 (18.3) | 375 (280.5) | - | - | 4 | - |
| NEMB | 160 (24.5) | 283 (226.5) | - | - | 1 | - | |
| Cobb et al., 201817 | EMB | - | - | 4.5 (1.2) | 3 | - | 0 |
| NEMB | - | - | 2 (0.6) | 3 | - | 2 | |
| del Guercio et al., 201318 | EMB | - | 320 (85) | - | - | - | - |
| NEMB | - | 255 (48) | - | - | - | - | |
| Gözen et al., 202019 | EMB | - | - | - | - | 3 | 7 |
| NEMB | - | - | - | - | 1 | 2 | |
| Gwon et al., 201120 | EMB | - | - | - | 3 | - | - |
| NEMB | - | - | - | 1 | - | - | |
| Ikeda et al., 201821 | EMB | 280.5 (74.96) | 385.2 (126.59) | - | 0 | - | 51 |
| NEMB | 287.2 (83.45) | 188.9 (112) | - | 1 | - | 10 | |
| Law et al., 201722 | EMB | 264 (161) | 530 (697) | - | 2 | 2 | - |
| NEMB | 269 (132) | 667 (628) | - | 0 | 0 | - | |
| Li et al., 201023 | EMB | 170.3 (75.4) | 354.8 (334.4) | 8 (2.1) | 1 | 3 | 1 |
| NEMB | 224.6 (114) | 656.4 (497.4) | 9.5 (3.5) | 3 | 4 | 4 | |
| Li et al., 202224 | EMB | 195.48 (111.97) | <30 mm: 55.9 (23.2) | - | 5 | 38 | 29 |
| >30 mm:202.6 (73.9) | |||||||
| NEMB | 205.64 (117.82) | <30 mm: 27.9 (9.4) | - | 3 | 13 | 11 | |
| >30 mm:312.5 (131.7) | |||||||
| Lim et al., 201025 | EMB | 360 (103.9) | 550 (301.4) | 8 (2.3) | - | - | - |
| NEMB | 355 (75.1) | 675 (353.9) | 8 (1.2) | - | - | - | |
| Liu et al., 201826 | EMB | 110.6 (35.8) | 140.3 (57.1) | 9.9 (2.1) | 1 | 8 | 2 |
| NEMB | 188.3 (66.4) | 396.4 (272.8) | 10.9 (3.7) | 2 | 13 | 4 | |
| Mohebali et al., 202027 | EMB | 198.33 (61.13) | 437 (545) | - | 0 | - | 0 |
| NEMB | 161.5 (55.56) | 262 (222) | - | 0 | - | 0 | |
| Mourad et al., 201628 | EMB | 34.9 | 105 | - | - | 10 | 4 |
| NEMB | 38.1 | 110 | - | - | 14 | 2 | |
| Osofsky et al., 202129 | EMB | 337 (195) | 242 (178) | 3.8 (2.9) | 1 | 2 | 8 |
| NEMB | 199 (100) | 242 (27) | 2.3 (2.1) | 1 | 2 | 2 | |
| Power et al., 201230 | EMB | 250 | 263 (250) | 4.1 | 0 | 8 | 21 |
| NEMB | 265 | 599 (265) | 4.2 | 1 | 40 | 32 | |
| Rao et al., 201731 | EMB | 102 | 120 | - | - | - | - |
| NEMB | 73.3 (9.9) | 131.2 (15.5) | - | - | - | - | |
| Sen et al., 201332 | EMB | - | - | - | 2 | - | 7 |
| NEMB | - | - | - | 0 | - | 4 | |
| Wernick et al., 202033 | EMB | - | 299 | - | - | - | - |
| NEMB | - | 205 | - | - | - | - | |
| Wu et al., 202234 | EMB | - | - | - | 1 | 2 | 10 |
| NEMB | - | - | - | 0 | 10 | 16 | |
| Yazman et al., 202235 | EMB | - | 217 (31) | 5.1 (0.4) | 1 | 4 | 5 |
| NEMB | - | 406 (45) | 6 (0.3) | 1 | 6 | 7 | |
| Zeitler et al., 201036 | EMB | - | 305 | - | - | 1 | 2 |
| NEMB | - | 265.6 | - | - | 1 | 2 | |
| Zhang et al., 201237 | EMB | 185 (17.6) | 365 (236.1) | 5.5 (1.2) | - | - | - |
| NEMB | 217.5 (26) | 500 (261.4) | 8.3 (1.5) | - | - | - | |
| Zhang et al., 201838 | EMB | 122.5 (14.5) | 85 (23.3) | - | - | 6 | 4 |
| NEMB | 161.8 (9.6) | 268.8 (115.3) | - | - | 6 | 4 |
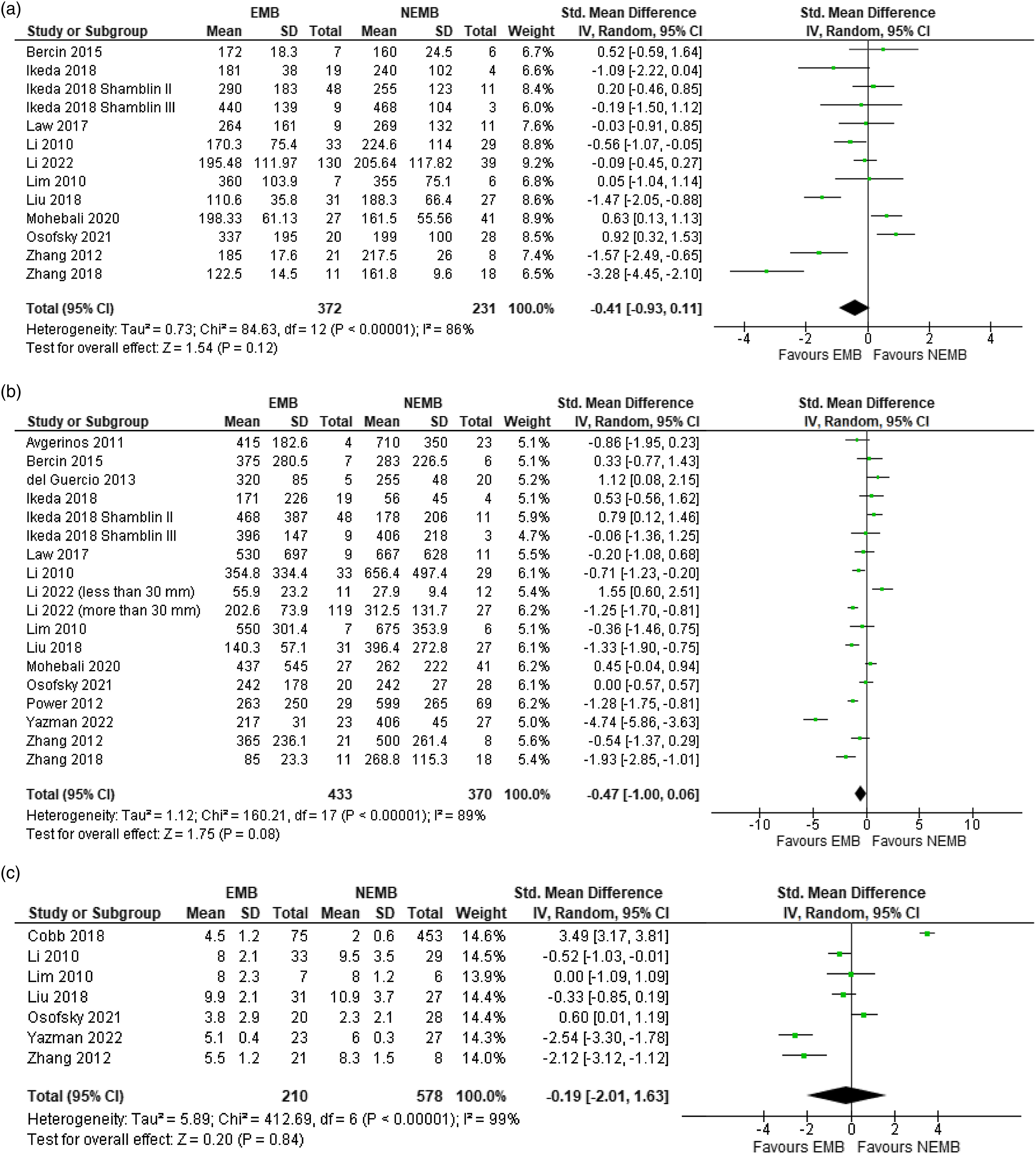
Operative Time
Intraoperative Blood Loss
Postoperative Hospital Stay
Perioperative Complications
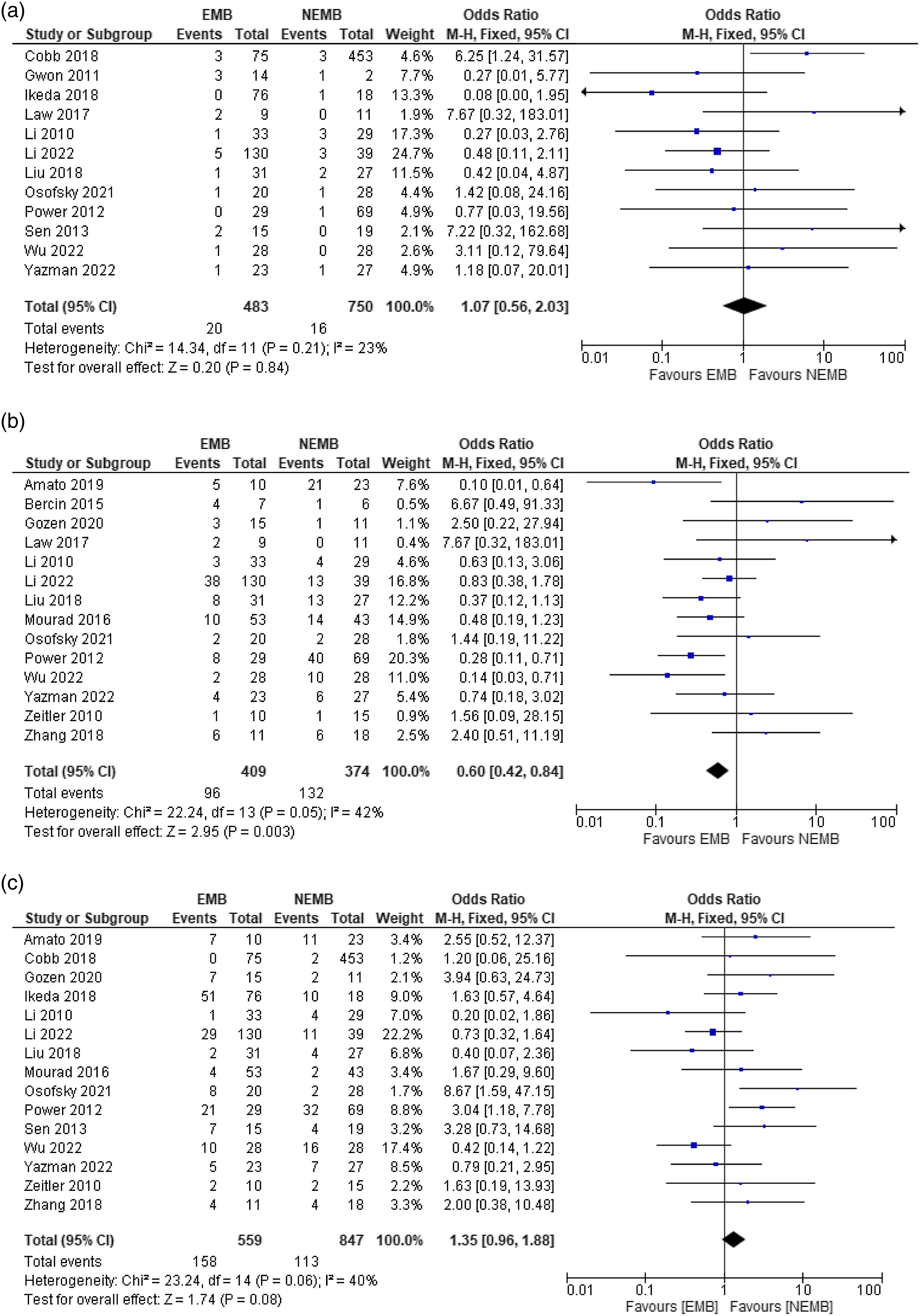
TIA/Stroke
Vascular Injury
Cranial Nerve Injury
Sub Analysis According to Shamblin Grade
Quality Assessment
| Selection | Comparability | Outcome | |
|---|---|---|---|
| Amato et al., 201914 | ✸✸✸ | ✸ | ✸✸ |
| Avgerinos et al., 201115 | ✸✸✸✸ | ✸ | ✸✸✸ |
| Bercin et al., 201516 | ✸✸✸ | ✸ | ✸ |
| Cobb et al., 201817 | ✸✸✸ | ✸✸ | ✸ |
| del Guercio et al., 201318 | ✸✸✸✸ | - | ✸✸ |
| Gözen et al., 202019 | ✸✸✸✸ | ✸ | ✸ |
| Gwon et al., 201120 | ✸✸✸✸ | - | ✸ |
| Ikeda et al., 201821 | ✸✸✸✸ | ✸ | ✸ |
| Law et al., 201722 | ✸✸✸✸ | - | ✸✸✸ |
| Li et al., 201023 | ✸✸✸✸ | - | ✸✸ |
| Li et al., 202224 | ✸✸✸ | - | ✸✸ |
| Lim et al., 201025 | ✸✸✸✸ | - | ✸✸ |
| Liu et al., 201826 | ✸✸✸✸ | ✸ | ✸✸ |
| Mohebali et al., 202027 | ✸✸✸ | - | ✸✸✸ |
| Mourad et al., 201628 | ✸✸✸ | - | ✸✸ |
| Osofsky et al., 202129 | ✸✸✸ | ✸ | ✸✸ |
| Power et al., 201230 | ✸✸✸✸ | ✸ | ✸✸✸ |
| Rao et al., 201731 | ✸✸✸ | - | ✸✸✸ |
| Sen et al., 201332 | ✸✸✸✸ | ✸ | ✸✸✸ |
| Wernick et al., 202033 | ✸✸✸ | - | ✸✸ |
| Wu et al., 202234 | ✸✸✸ | - | ✸✸ |
| Yazman et al., 202235 | ✸✸✸ | - | ✸✸ |
| Zeitler et al., 201036 | ✸✸✸ | - | ✸ |
| Zhang et al., 201237 | ✸✸✸✸ | - | ✸✸ |
| Zhang et al., 201838 | ✸✸✸ | - | ✸✸ |


Discussion
Limitations
Future Perspectives
Conclusion
Declaration of Conflicting Interests
Funding
ORCID iDs
Footnotes
References
Appendix A Complete search query.
| N | Query | Results |
|---|---|---|
| PUBMED 1033 | ||
| 1 | Search: Carotid body tumor + embolization/tumor embolization/preoperative embolization | 157 |
| ((carotid body tumor [MeSH terms]) OR (carotid body tumor) OR (carotid body tumors) OR (carotid body tumors [MeSH terms])) AND ((embolization, therapeutic [MeSH terms]) OR (embolization) OR (embolization) OR (embolism) OR (tumor embolization) OR (preoperative embolization)) AND (English [Language]) AND ((“2010/01/01” [Date - publication]: “2022/09/30” [Date - publication])) | ||
| 2 | Search: Paraganglioma + embolization/tumor embolization | 322 |
| ((Paraganglioma, carotid body [MeSH terms]) OR (paraganglioma, extra adrenal [MeSH terms]) OR (carotid body paraganglioma [MeSH terms]) OR (carotid body paragangliomas [MeSH terms]) OR (paraganglioma) OR (paragangliomas) OR (carotid paraganglioma) OR (carotid paragangliomas) OR (carotid body paraganglioma) OR (carotid body gangliomas)) AND ((embolization, therapeutic [MeSH terms]) OR (embolization) OR (embolization) OR (embolism) OR (tumor embolization) OR (preoperative embolization)) AND (English [Language]) AND ((“2010/01/01” [Date - publication]: “2022/09/30” [Date - publication])) | ||
| 3 | Search: Glomus carotid body tumor + embolization | 23 |
| (glomus carotid body tumor) AND ((embolization, therapeutic [MeSH terms]) OR (embolization) OR (embolization) OR (embolism) OR (tumor embolization) OR (preoperative embolization)) AND (English [Language]) AND ((“2010/01/01” [Date - publication]: “2022/09/30” [Date - publication])) | ||
| 4 | Search: Carotid body tumor + surgical resection/resection | 271 |
| ((Carotid body tumor [MeSH terms]) OR (carotid body tumor) OR (carotid body tumors) OR (carotid body tumors [MeSH terms])) AND ((surgical resection) OR (resection)) AND (English [Language]) AND ((“2010/01/01” [Date - publication]: “2022/09/30” [Date - publication])) | ||
| 5 | Search: CBT + ultrasonography/mediums | 260 |
| ((Carotid body tumor [MeSH terms]) OR (carotid body tumor) OR (carotid body tumors) OR (carotid body tumors [MeSH terms])) AND ((cyanoacrylate) OR (ultrasonography) OR (micronized tantalum powder) OR (ethylene vinyl alcohol copolymer)) AND (English [Language]) AND ((“2010/01/01” [Date - publication]: “2022/09/30” [Date - publication])) | ||
| Scopus 744 | ||
| 10 | TITLE-ABS-KEY (“carotid body tumor” OR “paragangliomas” OR “paraganglioma” OR “glomus carotid body tumor” OR “carotid body paraganglioma” OR “carotid paraganglioma” AND “embolization” OR “embolism” OR “surgical resection”) AND PUBYEAR >2009 AND PUBYEAR <2023 AND (LIMIT-TO ( LANGUAGE, “English”) ) | 744 |
| Web of Science 543 | ||
| 16 | ((TS = (carotid body tumor)) AND TS = (embolization)) AND DOP=(2010-01-01/2022-09-30) | 237 |
| 17 | ((TS = (paraganglioma)) AND TS = (embolization)) AND DOP = (2010-01-01/2022-09-30) | 242 |
| 18 | ((TS = (glomus carotid body tumor)) AND TS = (embolization)) AND DOP = (2010-01-01/2022-09-30) | 64 |
| Journals | ||
| 19 | European journal of vascular and endovascular surgery | 0 |
| 20 | Journal of vascular surgery | 0 |
| 21 | Angiology | 0 |
| 22 | Journal of cardiothoracic surgery | 0 |
| 23 | Journal of thoracic and cardiovascular surgery | 0 |
| 24 | European journal of cardiothoracic surgery | 0 |
| 25 | Annals of vascular surgery | 0 |
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In
Keywords
Rights and permissions
Authors
Metrics and citations
Metrics
Publication usage*
Total views and downloads: 2063
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 2 view articles Opens in new tab
Crossref: 4
- Multimodal Approach to the Management of a Carotid Body Tumor With Preoperative Direct Puncture Embolization Followed by Surgical Resection: A 2-Dimensional Operative Video
- Current Understanding of Carotid Body Paraganglioma Management
- Surgical Resection of a Shamblin Type III Carotid Glomus Tumor Without Preoperative Embolization: A Case Report
- Carotid body tumors—epidemiology and surgical resection
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.
