

Exploring Afghan Refugees’ Post-Resettlement Experiences in North America: A Scoping Review
Abstract
Background
Objective
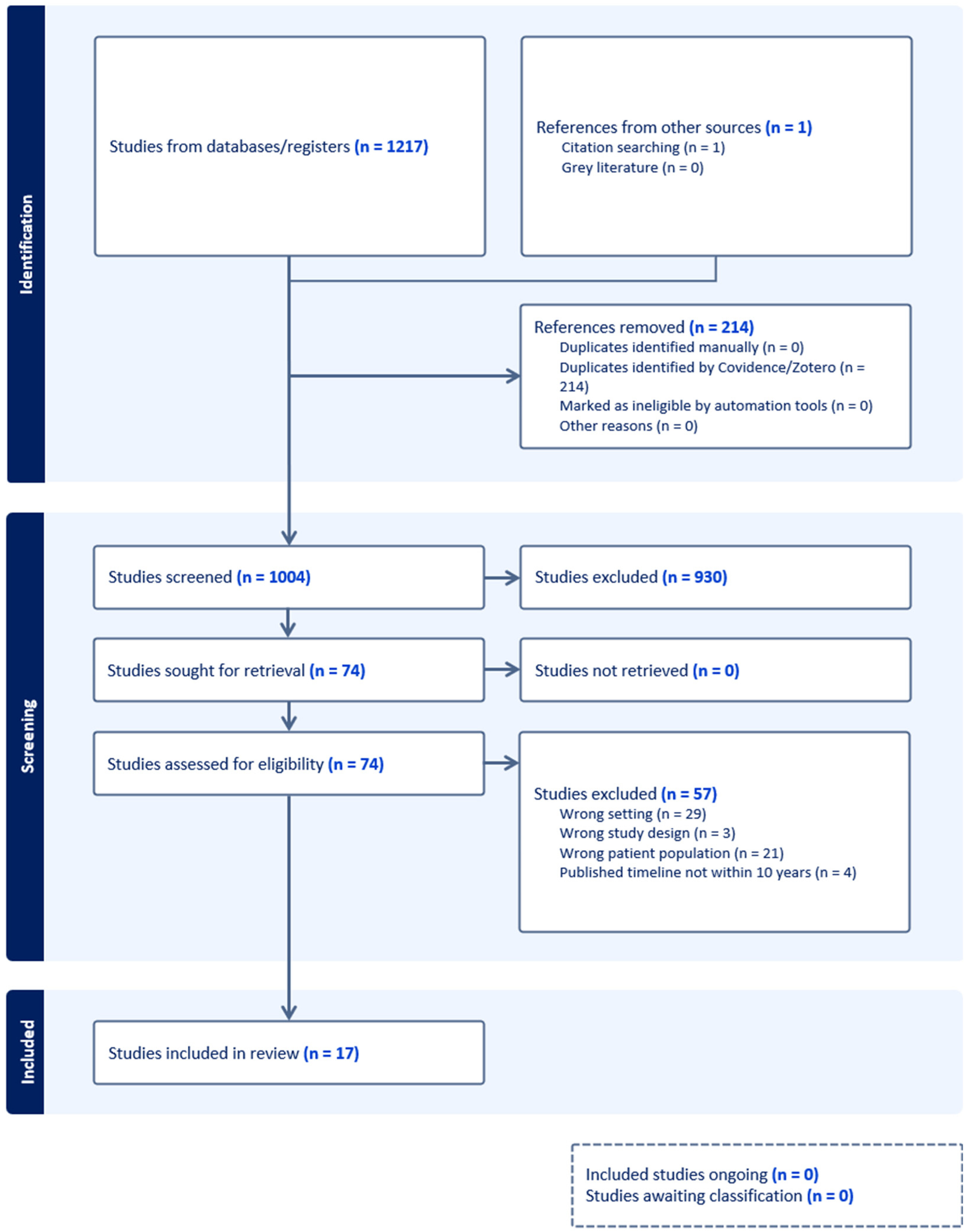
Methods
Results
Conclusion
Background
Materials and Methods
Search Strategy
| Database | Search Strategy | Results |
|---|---|---|
| CINAHL | (MH “Refugees”) AND (MH “Afghan persons”) AND (experiences OR challenges OR barriers OR difficulties) | 0 |
| (MH “Refugees”) AND (MH “Afghan persons”) | 25 | |
| EBSCOhost | (Afghans OR Afghan) AND (migration OR immigration OR emigration OR refugee) AND resettlement refugee) | 16 |
| EMBASE | Afghan* AND (refugee OR immigra* OR migra* OR emigra* OR settlement OR resettlement) AND (experiences OR challenges OR barriers OR difficulties) | 126 |
| Medline | Afghan* AND (refugee OR immigra* OR migra* OR emigra* OR settlement OR resettlement) AND (experiences OR challenges OR barriers OR difficulties) | 173 |
| Proquest | Afghan AND refugees AND (experiences OR challenges OR barriers OR difficulties) | 576 |
| Pubmed | Afghan* AND (refugee OR immigra* OR migra* OR emigra* OR settlement OR resettlement) AND (experiences OR challenges OR barriers OR difficulties) | 326 |
| Total | 1217 |
| Authors and Year | Country | Topic | Aim | Method | Population and Sample Size | Results |
|---|---|---|---|---|---|---|
| Soltan et al. (2023) | Canada | Acculturation | Examine impact of acculturation gaps between Afghan refugee young adults and their parents on family relationships, adaptation outcomes, and subjective wellbeing in Canada. | Qualitative | 148 participants: 77 emerging adults, 68 parents, and 3 caregivers | Emerging adults in Afghan refugee families who maintained proficiency in Farsi and a strong Afghan cultural identity experienced better mental health and family relationships. Parents’ acculturation to Canadian culture significantly supported their children's psychological adaptation. A large gap in Canadian identity between parents and emerging adults led to poorer family cohesion and increased intergenerational conflict. |
| Goliaei et al. (2023) | U.S. | Food Security | Investigate Afghan refugees’ food access and insecurity in the San Joaquin Valley, California. | Qualitative | 12 key informants and 12 Afghan refugee families | Afghan refugee newcomers faced significant challenges accessing food due to unfamiliarity with grocery store systems, limited transportation, high costs, and a lack of culturally or religiously appropriate options (halal food). Many avoided food banks because the items provided did not meet their dietary restrictions. They expressed a need for better financial literacy support and access to affordable, culturally suitable groceries. |
| Abuali et al. (2024) | U.S. | Health Profile | Understand the physical and psychosocial health needs of newly arrived Afghan refugee children. | Retrospective study | 121 recent Afghan refugee children | A review of 121 patient charts revealed high rates of health issues among Afghan refugee children, including malnutrition (25%); dental caries (74%); treatable infectious diseases such as schistosomiasis, strongyloidiasis, tuberculosis, and leishmaniasis; and mental health symptoms. Most parents and children did not speak English, and barriers to healthcare access included limited English proficiency and lower parental education levels. |
| Siddiq et al. (2022) | U.S. | Healthcare Access and Experiences | Explore sociocultural factors that influence mammography and colonoscopy screening behaviors among Afghan refugee women. | Focused ethnography design | 19 Afghan women over the age of 50 | Afghan refugee women often perceived cancer as a fatal disease, leading to fear, shame, and avoidance of preevntive screening. This was influenced by negative healthcare experiences, such as miscommunication and language barriers. However, support from family, reminders from providers, care by female practitioners, and spiritual coping strategies like duaa fostered resilience and encouraged engagement in cancer screening. |
| Siddiq et al. (2023) | U.S. | Healthcare Access and Experiences | Explore older Afghan refugee women's perceptions of individual and sociocultural factors of health and health care experiences. | Focused ethnography design | 14 Afghan women over 50, 5 family members, 8 community informants | Older Afghan refugee women's health experiences were shaped by five themes: health promotion thrrough religion, central role ofd family, ongoing displacement stressors, challenges navigating the health care system, and miscommunication from healthcare providers. |
| Worabo et al. (2024) | U.S. | Healthcare Access and Experiences | Investigate Afghan women's maternal health experiences in South Texas. | Qualitative descriptive design | 20 Afghan women who gave birth in the US within the past 2 years | Afghan refugee women in the U.S. reported largely positive maternal healthcare experiences, which contrasts the challenges they experienced in Afghanistan. They shared preference for female provideres, need for contraceptive education, and difficulties navigating the healthcare system. Some shared concerns about poor birth outcomes, language barriers, and structural barriers (e.g., transportation, finances). |
| Rosenberg et al. (2022) | U.S. | Healthcare Access and Experiences, Mental Health | Identify potential interventions to increase access to needed care and services for Afghan refugee children. | Community-based participatory research, grounded theory | 10 recently-arrived Afghan refugee families (9 mothers and 10 fathers) | Four themes: a shift in parental focus toward children's development as safety improved; acculturation stress related to technology use and preserving traditions; gradual adjustment to the U.S. support system amidst feelings of isolation; and growing trust in the more involved and coordinated U.S. healthcare system. |
| Rosenberg et al. (2024) | U.S. | Healthcare Access and Experiences, Mental Health | Analyze the perspectives and experiences of Afghan families and refugee-serving stakeholders regarding mental health program. To determine factors of successful implementation of preventive mental health intervention. | Qualitative thematic analysis | 6 refugee-serving stakeholders and five refugee parents. | Five key themes were identified in supporting refugee families: cultural humility and mutual learning in discussing emotions; adequate support networks; foster multidirectional communication among children, families, and educators; differing perspectives between families and stakeholders on intervention outcomes; and timely, culturally-informed interventions. |
| Quirke (2014) | Canada | Information practices | Explore the information practices of Afghan newcomer youth in Canada, focusing on two contexts: leisure activities and settlement. | Qualitative Exploratory | 7 Afghan newcomer youth in Canada (ages 12 to 24) | Afghan newcomer youth in Canada experienced significant challenges in accessing information due to language barriers, unfamiliar systems, and social isolation, often relying on informal networks and technology. Their leisure activities were shaped by cultural tensions and adaptation struggles, highlighting the need for more culturally responsive and accessible information services. |
| Alemi et al. (2015) | U.S. | Mental health | Investigate psychological distress symptoms and examine variables that correlate with and predict psychological distress levels among Afghan refugees. | Cross-sectional | 130 Afghan refugees (74 males and 56 females) | Low levels of distress observed in this sample, possibly reflecting improved safety. Symptoms like insomnia, headaches, and irritability were common. Factors that predicted distress: female, widowed, financial difficulties, disabled, and low education attainment. Factors that did not predict distress: acculturation, perceived social support |
| Alemi and Stempel (2018) | U.S. | Mental health | Investigate effects of perceived discrimination, distress, and post-settlement factors on the mental health of Afghan refugees. | Cross-sectional | 250 Afghan resettled refugee adults | Higher psychological distress was significantly related to perceived discrimination, pre-resettlement trauma, and strong intra-ethnic identity. Social support and ethnic integration reduced distress. |
| Stempel et al. (2016) | U.S. | Mental health | Examine the moderating/mediating effects of gender on distress and resilience among Afghan refugees. | Cross-sectional | 259 Afghan refugee adults | Higher distress levels were significantly associated with perceived discrimination, pre-resettlement trauma, and dissonant acculturation. English proficiency and family ties offer protective effects, especially for women. Gender ifferences revealed that English ability reduced distress more for women, while traditional gender ideologies and extended family ties increased distress for men. |
| Ahmad et al. (2020) | Canada | Mental health | Explore effects of social support, coping on PTSD symptoms among Afghan refugees in Canada. | Cross-sectional | 49 Afghan refugees adults resettled in Canada | PTSD prevalence in this sample was 53.1%, higher among those who were older, unemployed, and self-reported poor/fair health. Increased perceived social support significantly buffered PTSD symptoms and was associated with better coping and self-rated health. |
| Kirsch et al. (2024) | U.S. | Mental Health | Explore the relationship between collective trauma and mental health outcomes within Afghan refugee population. | Mixed method: Community-based participatory research, cross-sectional | 173 recently resettled Afghan refugees | Trauma and mental health outcomes varied by visa status, gender, displacement, English proficiency, and income level. Humanitarian parolees, women, low-income individuals, and minority ethnic groups experienced higher levels of mental health symptoms and traumas. |
| Alemi et al. (2017) | U.S. | Mental health | Investigate beliefs about depression among Afghans residing in the San Diego area. | Qualitative | 93 Afghan refugees (50 men and 43 women) | Both genders shared core beliefs about causes, risk factors, and treatments for depression. Women identified more causes and symptoms and favored religious or herbal remedies, while men linked depression to cultural elements like Afghan music and their gender. Women showed greater cultural knowledge and reported higher psychological distress related to socioeconomic and acculturation challenges. |
| Alemi et al. (2016) | U.S. | Mental health | Examine how Afghan refugees conceptualize depression and describe their experiences with depressive symptoms. | Qualitative descriptive approach | 18 Afghan refugee adults (11 males, 7 females) | Afghan refugees reported pre-migration traumas such as war, family separation, and difficult journeys, compounded by post-resettlement stressors including cultural adjustment, financial hardship, housing issues, and loss of Afghan identity and values. Depression was described using culturally specific terms and linked to both physical and psychological consequences. Coping strategies emphasized family unity, social connection, prayer, and finding purpose through their children's successes. |
| Nourpanah (2014) | Canada | Social Integration | Analyze how government-assisted Afghan refugees adapt to life in Canada. | Qualitative | 10 Afghan government-assisted refugees | Afghan families in Canada maintained strong visual and cultural ties to their heritage while also adapting to new social norms. Mutual accommodation and negotiation between parents and children on issues such as religion, gender roles, and education. Expression of religiosity varied as some families found comfort and identity in faith, while others distanced themselves from religion, viewing it as a symbol of past constraints. |
Inclusion and exclusion criteria
Selection Process and Data Extraction
Data Analysis
Results
Mental Health
Psychological Distress
Depression
Post-Traumatic Stress Disorder
Health Status, Healthcare Practices, and Healthcare Experiences
Other Post-Migration Challenges
Discussion
Limitations
Conclusion
Declaration of Conflicting Interests
Funding
ORCID iDs
Data availability statement
References
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In

Keywords
Rights and permissions
Data availability statement
Article versions
Authors
Metrics and citations
Metrics
Journals metrics
This article was published in Canadian Journal of Nursing Research.
View All Journal MetricsPublication usage*
Total views and downloads: 565
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 0
Crossref:
There are no citing articles to show.
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.
