Introduction
Cardiovascular disease (CVD) remains the primary cause of mortality in Canadian women,
1,2 with deaths from adverse cardiac events rising in women over the past 5 decades.
3 Despite recent advances in cardiac care, the current methods used for cardiovascular risk stratification in women perform poorly, particularly in younger women.
4,5 The most common means of risk stratification, such as the Framingham Risk Score, have been demonstrated to underestimate cardiovascular risk in women.
4,5 There is an ever-increasing need for improved risk stratification in women that also considers sex-specific risk factors in addition to traditional cardiovascular risk factors (
Table 1).
6-9 Prior studies have also shown that obesity and lifestyle factors such as lack of exercise, increased stress, and an unbalanced diet, as well as medical comorbidities such as diabetes, autoimmune disorders, and chronic kidney disease disproportionately confer increased cardiovascular risk in women of reproductive age relative to men.
9 Diabetes in particular has been found to have a larger risk-enhancing effect in women relative to men.
10 Furthermore, the majority of Canadian women are unaware of their personal cardiovascular risk and factors that influence their risk for adverse cardiovascular events.
2,11Evidence of an association between the presence of breast arterial calcifications (BAC) on mammography, the presence of coronary artery calcifications (CAC), and increased cardiovascular risk is growing.
12,13 In several studies, BAC has been identified as an independent marker of cardiovascular risk status,
14-20 particularly in younger women.
21 BAC has been demonstrated to correlate with other methods of cardiovascular risk stratification, including the Framingham Risk Score, Pooled Cohort Equation Risk Score, and CAC scores, among others.
15-17,22-30 However, many of the traditional risk stratification scoring systems do not take into account sex-specific risk factors for women.
31Perimenopausal and postmenopausal women are at an increased risk of adverse cardiovascular events secondary to reduced levels of serum estrogen and thus, a decrease in the cardioprotective effects of estrogen.
32-35 Circulating estrogen reduces cardiovascular risk by improving cardiovascular function, slowing or preventing the development of cardiac hypertrophy, reducing coronary arterial atherosclerosis, and protecting against reperfusion injury in those with myocardial ischemia.
33 Just as there are sex-specific cardiovascular risk factors for women that differ from traditional cardiovascular risk factors, the signs and symptoms of acute coronary syndrome (ACS) are also different between men and women. Women with myocardial infarction (MI) are more likely to present with atypical symptoms such as epigastric pain or gastrointestinal upset rather than typical angina described as retrosternal chest pain triggered by exercise and relieved with rest (
Table 2).
33,36Given the significant overlap in populations of perimenopausal and postmenopausal women and those undergoing screening mammography,
37 the reporting of BAC on mammography has the potential to also identify women at higher risk of cardiovascular events where early initiation of optimal medical management as a preventative health strategy could improve health outcomes. This manuscript provides a comprehensive review of the literature linking BAC with higher cardiovascular event risk, description and quantification of BAC, radiologist awareness and reporting habits, and preferences of referring physicians and patients undergoing screening mammography.
Prevalence and Clinical Significance of Breast Arterial Calcifications in the Population
The prevalence of BAC on screening mammography has been reported to be 12% to 43% and increases with advancing age.
15,16,23,26,28,38,39 BAC positively correlates with CAC, coronary artery disease (CAD), and subclinical or asymptomatic CVD.
20 Kemmeren et al determined that, in women over 50 years of age, the presence of BAC on mammography is associated with an increased risk of cardiovascular death. This risk was further increased in those with known diabetes.
40 Furthermore, the lack of BAC on mammography has been found to be a strong negative predictor for the absence of severe CAC or clinically significant CAD.
16,39 Obstructive CAD was positively correlated with BAC, however, the grading severity of BAC was not significantly associated with increased likelihood of CAD in one study.
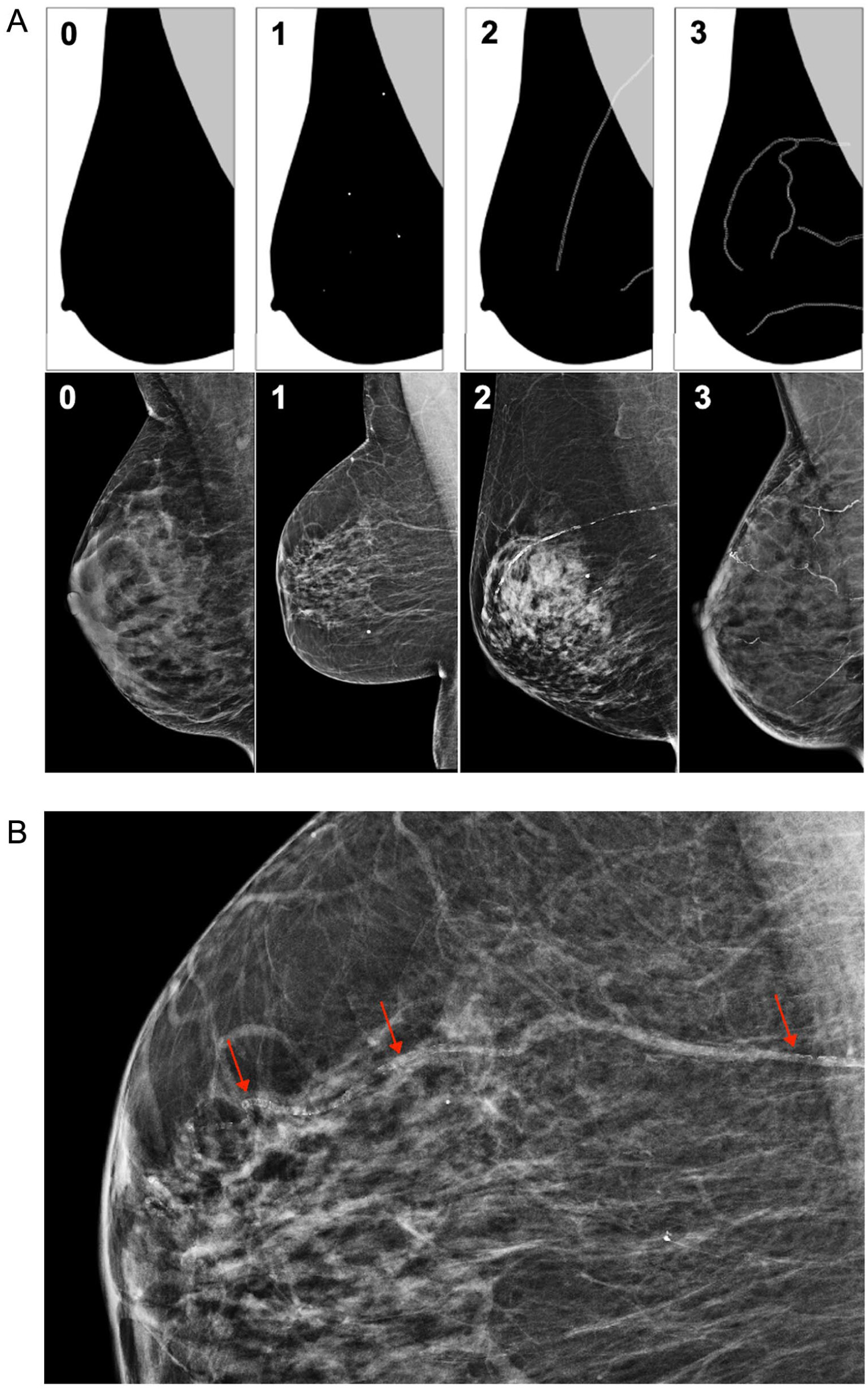
16 In contrast, Mostafavi et al found that moderate to severe BAC is correlated with moderate to severe CAD as visualized on coronary CT angiography, based on a predetermined 4-point grading system (
Figure 2).
38 The heterogeneity in findings between studies examining breast arterial calcification (BAC) and coronary artery disease (CAD) likely reflects the differences in population characteristics between the 2 studies, as both used similar BAC scoring systems. McLenachan et al
16 studied 405 women from the SCOT-HEART trial, all symptomatic patients with suspected stable angina referred for coronary CTA, whereas Mostafavi et al,
38 included 100 women (both symptomatic and asymptomatic) who underwent coronary CTA for a variety of clinical indications. The SCOT-HEART cohort had lower BAC prevalence (12% compared to 23%) and represented a pre-selected symptomatic population, which may have diluted the discriminatory power of BAC for identifying asymptomatic obstructive disease.
In addition to CAD, patients with BAC are also more likely to have hypertension, hyperlipidemia, diabetes mellitus, and metabolic syndrome.
16,28,29,40 BAC has also been correlated with other systemic illnesses including peripheral vascular disease, chronic kidney disease, and osteopenia.
26,28,32,41,42 Patients with BAC are more often postmenopausal, less likely to have used hormone replacement therapy, and multiparous.
26 Conversely, BAC has been demonstrated to be negatively correlated with alcohol consumption and smoking.
16,26There is also evidence that the presence of BAC on mammography is linked to the development of clinically significant heart disease. Patients with BAC were found to have an increased frequency of critical coronary artery stenosis and higher CAC scores.
39 A 2012 meta-analysis found that patients with BAC had an increased likelihood of having CAD at coronary angiography.
43 Moreover, in patients without a diagnosis of CAD or ischemic heart disease, those with BAC were more likely to develop ischemic heart disease or ischemic stroke than those without BAC on mammography, despite controlling for age.
27,44 A study by Sedighi et al discovered that BAC was correlated with an increased risk of carotid atherosclerosis.
45 The Multiethnic Study of Breast Arterial Calcium Gradation and Cardiovascular Disease (MINERVA study) found that the presence of BAC on mammography is associated with an increased risk of global CVD and atherosclerotic cardiovascular disease (ASCVD) including MI, ischemic stroke, and death due to CVD.
46,47 The MINERVA study suggests that BAC can be used as a potential screening method of subclinical CVD and correlates with cardiovascular events.
46,47 Newallo et al found that BAC on mammography in a cohort of African American patients had a specificity of 85% for a CAC score of greater than 100; this is equivalent to a 50% to 69% or greater (moderate) stenosis with or without flow limitation or plaque burden with moderate non-obstructive CAD considered highly likely.
48-51While there is a correlation between BAC and CAC, the pathophysiology resulting in BAC differs from that of CAC.
15,17,45-47,52 BAC are the result of circumferential calcifications of the vessel media resulting in vascular stiffness or inelasticity, whereas CAC typically arise from calcifications of the vessel intima and result in eccentric luminal narrowing.
15,45,47,52 Medial calcifications, also referred to as medial calcific sclerosis, occur in small to medium-sized vessels and are more frequently associated with chronic renal disease, hypertension, peripheral arterial disease, and diabetes; intimal calcifications are those often seen in the larger vessels (eg, coronary and carotid arteries) of those who smoke or have hyperlipidemia.
15,41,45,46,52 Calcification of the arterial tunica media is independent of lipid deposition seen with calcifications of the tunica intima and may result in endothelial dysfunction, leading to altered flow and vessel remodelling.
17,47,52 Due to these effects, medial calcifications, such as those seen with BAC, can exacerbate ischemia in patients with concomitant atherosclerotic intimal calcifications or lead to cardiac failure.
17,52 Overall, there is significant evidence supporting a link between BAC, the various manifestations of CVD, and relevant comorbidities despite different pathophysiology.
Identifying and Quantifying Breast Arterial Calcifications
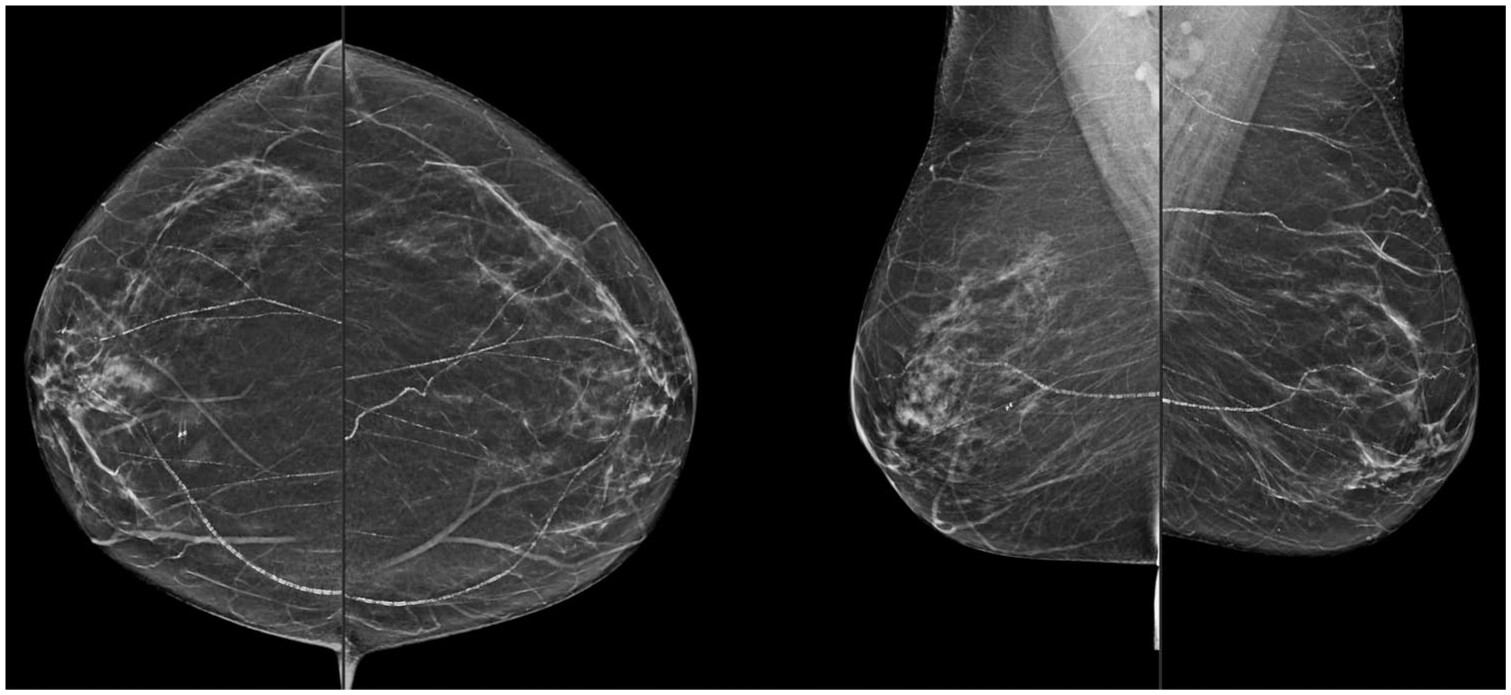
The detection and quantification of BAC on mammography can be performed subjectively by the interpreting radiologist. Depending on their severity, BAC may appear as coarse, tram-track, or tubular calcifications on mammography (
Figure 1).
16,38 BAC are often clearly distinguishable from other benign and suspicious microcalcifications by their morphology and proximity to breast vasculature. While BAC reporting is not required based on the American College of Radiology (ACR) Breast Imaging Reporting and Database System (BI-RADS) 5th edition guidelines, radiologists may choose to describe vascular calcifications when reporting mammography.
53Radiologists may comment on the presence of BAC on mammography via a binary assessment (BAC are present or absent) or via subjective or semi-quantification (eg, none, mild, moderate, or severe), either based on the number of calcified vessels or visual assessment of calcium density (
Figure 2).
16,17,38,54-58 Other studies have proposed lengthier scoring scales which consider the number and length of calcified breast arteries and subjective visual assessment of calcium density.
46 Several studies have explored the utility and feasibility of measured quantification of BAC on mammography via densitometry and machine learning.
46,59,60 One densitometry model for BAC found that the calcifications were overestimated in fatty breasts and underestimated in dense breasts, however, results of this study otherwise demonstrated adequate feasibility.
59The use of artificial intelligence (AI) in the detection and quantification of BAC on mammography has also been an area of increasing interest and development over the past several years. AI-based BAC detection and quantification models have been developed and assessed on both full-field digital mammography (FFDM) and digital breast tomosynthesis (DBT),
61 including the use of a transfer learning approach for the detection of BAC,
57 detection and densitometry measurements of BAC on mammography,
3 and convolutional neural networks to distinguish BAC from nonvascular breast calcifications.
60 The development of AI-based CVD risk models incorporating the presence or grading of BAC are also an area of recent development.
12While there have been several proposed methods of quantifying BAC on mammography, binary assessment or subjective quantification on a 4-point scoring system (eg, none, mild, moderate, or severe) currently remain the least time-consuming methods for radiologists reporting mammography while still conveying their presence and significance. More advanced methods, including semi-quantitative methods or AI-based models, have the potential to augment BAC identification and reporting, however, further studies are needed to determine the clinical and logistic utility of implementing such technology.
Radiologist Awareness and Reporting
Reporting of BAC amongst radiologists is heterogeneous across the United States, Europe, and Canada based on the results of 4 surveys from the 3 jurisdictions (
Table 3). An American survey study of radiologists through the ACR found that the most frequent follow-up recommendation made on mammography reports with BAC was primary care follow-up.
22 An additional American survey through the Society of Breast Imaging revealed that while the majority of radiologists were aware of the association between BAC and CAD, less than half of radiologists agreed that identification of BAC added value to screening mammography and only 0.7% consistently provided follow-up recommendations.
62Over half of Canadian radiologists are aware of the relationship between BAC and cardiovascular risk. However, only 16% routinely report their presence on mammography.
63 A subset of radiologists (35%) indicated that they occasionally report the presence of BAC in young patients or if the calcium burden is subjectively high.
63 Of those who report BAC on mammography, only 4% provide follow-up or management recommendations and 1% directly inform the patient.
63 There was consensus amongst surveyed Canadian radiologists that national BAC reporting guidelines are needed, with only 4% of responding radiologists indicating that their local radiology department or group had already established standards for reporting BAC.
63 Similar to breast tissue density, there were calls for increased awareness about the importance of BAC as a risk marker for CAD. However, despite these results, there are currently no outcome data to demonstrate that BAC reporting leads to improved long-term outcomes.
The discrepancy between awareness of the relationship between BAC and CAD and the low reporting rate has not been explicitly explored, but may be due to high workflow demands, unclear real-world clinical outcomes or benefits, and a lack of clear reporting and management pathways.
Preferences of Referring Physicians
Results of North American survey studies suggest that referring physicians would like to be made aware of the presence of BAC on mammography (
Table 4).
64,65 Some degree of quantification was favoured by referring physicians, and most physicians (80%) reported that the documentation of BAC on mammography would result in further assessment of a patient’s cardiovascular risk.
64 A minority of responding physicians indicated that they would pursue further cardiovascular workup with either CAC scoring CT (22%) or electrocardiography or stress test (16%).
64 However, data obtained from the BEACON study by McKee et al do not suggest that calcium score CT is needed in all patients found to have BAC.
66 Rather, the presence of BAC should prompt CVD risk assessment to guide further work-up and management. Specialist physicians who referred the patient for mammography indicated that they would defer the decision to pursue further investigations to the patient’s primary care physician, most of which indicated that they would disclose the presence of BAC to their patients.
64A Canadian survey of referring physicians conducted in 2023 found that a large proportion of surveyed physicians (83%) were unaware of the correlation between BAC and increased cardiovascular risk.
65 However, just over half of responding referring physicians preferred reporting of BAC on mammography, with 58% indicating that BAC reporting would result in implementation of risk mitigation strategies.
65 Most surveyed physicians (71%) stated that there was a need for national guidelines on the reporting and management of BAC, and 63% stated that they would disclose the presence of BAC and discuss their implication with patients.
65 Commentary left by referring physicians participating in the survey stressed the need for risk/benefit discussions with patients and shared decision-making as to the best course of action in the subsequent management of BAC and cardiovascular risk factors. Factors such as a patient’s age and comorbidities also factored into the substance of several comments, suggestion that stratification based on age and additional CVD risk factors in relation to the burden of BAC may be valuable to referring physicians.
Patient Preferences
An overwhelming majority (95.8%) of patients surveyed in a 2019 American study by Margolies et al expressed a desire to be made aware of the presence of BAC on mammography to guide informed decision making.
67 Approximately 22% of the surveyed patients were familiar with BAC prior to taking the survey.
67Patients were also surveyed on their preference for subsequent preventative measures or follow-up care following the detection of BAC on mammography. Lifestyle modifications such as changes to nutrition and exercise were selected by 34.1% of respondents; 14.7% of which indicated they would make such changes without formal involvement or guidance from their physician.
67 12.7% indicated they would commence prescribed medication without further evaluation with coronary artery CT.
67 Just over half (53.2%) of responses indicated a preference for further evaluation with coronary artery CT prior to planning further care.
67 Of the patients who preferred to undergo further evaluation with coronary artery CT, commencing prescribed medication (13.2%) and lifestyle changes (30.6%) would be considered if their CT should evidence of CAC; 56.3% of respondents would consider both medication and lifestyle modifications.
67A 2023 survey of patients by Vincoff et al evaluated the impact of direct patient notification of BAC on subsequent motivation to seek preventative care and the perceived value of BAC reporting.
68 Most participants (57.1%) discussed the presence and implications of BAC with their physician. Furthermore, 81% indicated that direct BAC notification was “very helpful” or “somewhat helpful,” with the majority (76.2%) responding in favour of routine patient notification of BAC on mammography.
68 This strongly suggests that patients desire information and greater autonomy pertaining to their overall health status, and that direct BAC notification may promote cardiovascular risk awareness and encourage patients to seek preventative care.
A 2025 prospective study by McKee et al found high rates of follow-up with primary care providers and increased adoption of lifestyle modifications following notification of the presence of BAC on mammography and CAC on calcium score CT in patients without previously-known CVD.
66 Most patients with BAC and CAC (92%) had an appointment scheduled with their primary care physician within 6 months of completing their mammogram; of those who attended the appointment, 44% were referred to cardiology and 17% were sent for electrocardiogram.
66 Forty-six percent of patients with both BAC and CAC had already implemented lifestyle modifications.
66 However, although this study notified patients of the presence of both BAC and CAC, 86% of participants with BAC and without CAC pursued follow-up with their primary care physician, highlighting the need for follow-up recommendations based on the presence of BAC.
66 Although calcium score CT was performed in all study subjects by McKee et al to assess for correlation between the presence of severity of BAC and CAC, the authors recommend initiation of cardiovascular risk assessment rather than routinely obtaining calcium score CT following the identification of BAC on mammography.
66 The calcium score CT may be completed to aid cardiovascular risk assessment in certain women who are at intermediate risk for CAD, to further risk stratify into low or high-risk groups and determine if lipid-lowering therapy should be initiated.
69When considering patient notification of BAC on mammography, it is important to remember the immense administrative workload of referring physicians, particularly family doctors. Given this large administration burden and triaging of results, incidental findings of BAC may be overlooked.
70 It may be beneficial to patients and physicians alike to consider direct patient notification of BAC, akin to standardized reporting of breast density, via a lay letter.
63 Consideration should also be made to the increasingly widespread rapid access that patients have to their medical imaging results in the age of electronic health records (EHR) and patient portals. Inclusion of basic information about BAC, its association with cardiovascular risks, and some recommended lifestyle modifications may empower patients to prioritize cardiovascular health and risk reduction. However, consideration should also be made to the potential for increased patient anxiety, similar to those risks touted by some regarding breast density notification.
63,71 Future investigations into the preferences of Canadian patients may provide further insight into the implications of BAC reporting and subsequent actions taken in the Canadian context. Despite all these factors, the intention of BAC reporting and patient notification would ultimately be to allow for patient autonomy and identify opportunities to improve cardiovascular health in women.
Potential Impact on the Healthcare System
Discussion on the benefits of reporting BAC on mammography is not complete without acknowledging the potential impact of widespread reporting on an already-stretched Canadian healthcare system. Although most women undergoing screening mammography will not have BAC, careful coordination, and clear communication between radiologists, family physicians and other primary care providers, cardiologists, and oncologists surrounding the reporting and management of BAC is critical to prevent an increase in administrative burden and unnecessary referrals.
66 Reporting of BAC may result in an increase of cardiology referrals, raising potential for capacity issues. As such, the decision to report BAC on mammography should be made in collaboration with regional referring physicians. However, by ensuring engagement by all relevant and involved parties, providing education, and creating robust and context-specific BAC reporting and management recommendations, the healthcare system in most instances will not be overwhelmed as most patients will not have BAC requiring any further workup or testing.
66 This is of particular importance given the high proportion of referring physicians who were unaware of the significance of BAC.
65 Reporting and clinical management recommendations can guide radiologists and referring physicians to ensure appropriate resource allocation and reduce the potential burden BAC reporting. However, given the general lack of awareness of BAC amongst Canadian referring physicians, any published recommendations must be accompanied by educational materials for primary care providers and referring physicians to minimize undue burden on the healthcare system.