Catheter placement
•
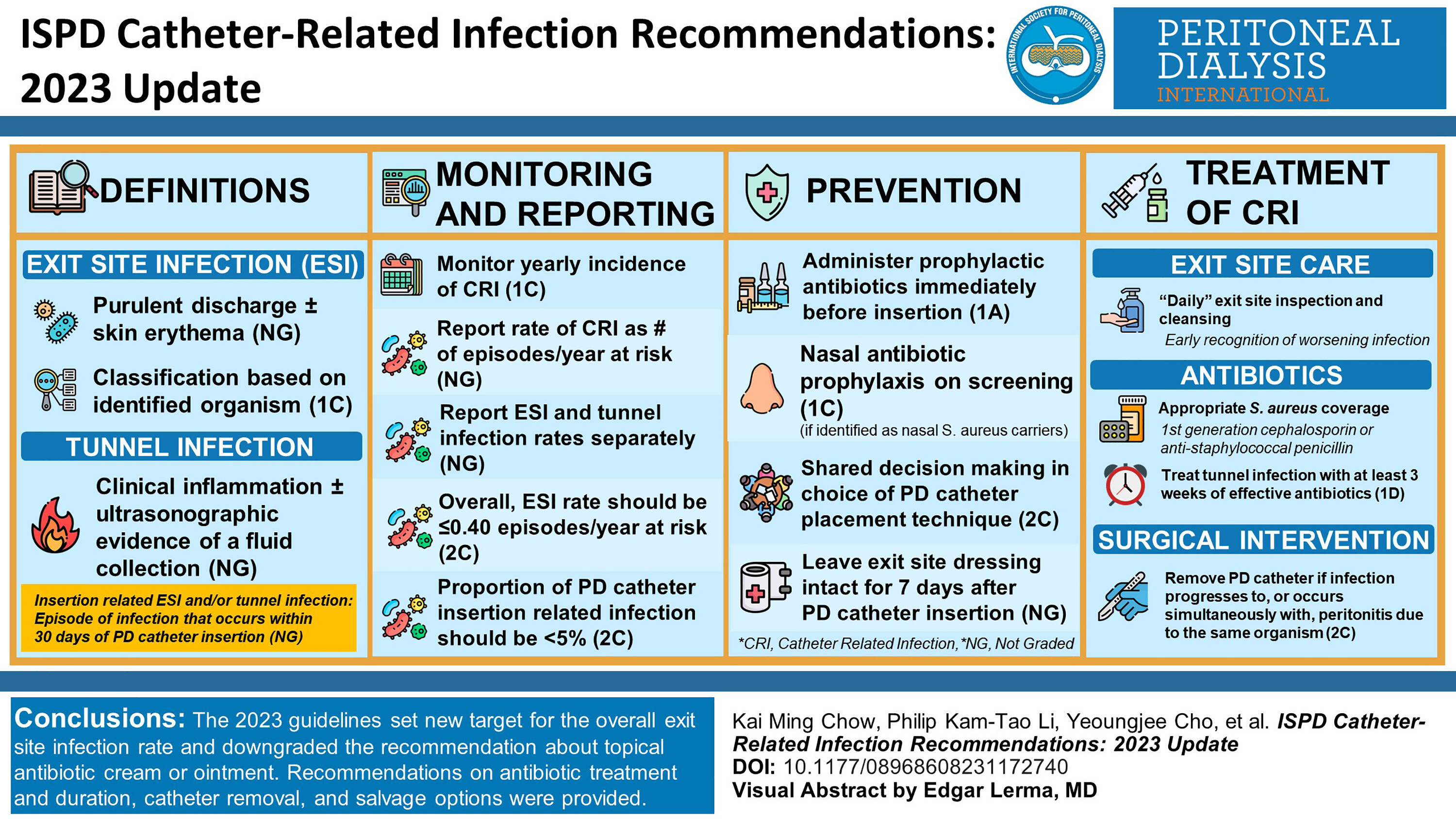
We recommend that prophylactic antibiotics be administered immediately before catheter insertion for prevention of peritonitis (1A), although their effects on catheter-related infections are uncertain.
•
We recommend the use of nasal antibiotic prophylaxis if patients are identified as being nasal S. aureus carriers on screening prior to PD catheter insertion (1C).
•
We suggest that choice of PD catheter placement technique be left to shared decision-making between the individual clinician and patient as the comparative efficacies and safety of reported catheter placement techniques for the prevention of catheter-related infections are uncertain (2C).
•
We suggest that the exit site dressing should be left intact for 7 days after PD catheter insertion, unless soiled, to immobilise the new catheter and reduce risk of infection (Not Graded).
The recommended practice and standard of PD catheter insertion has been detailed in the 2019 ISPD guideline on Creating and Maintaining Optimal Peritoneal Dialysis Access in the Adult Patient.
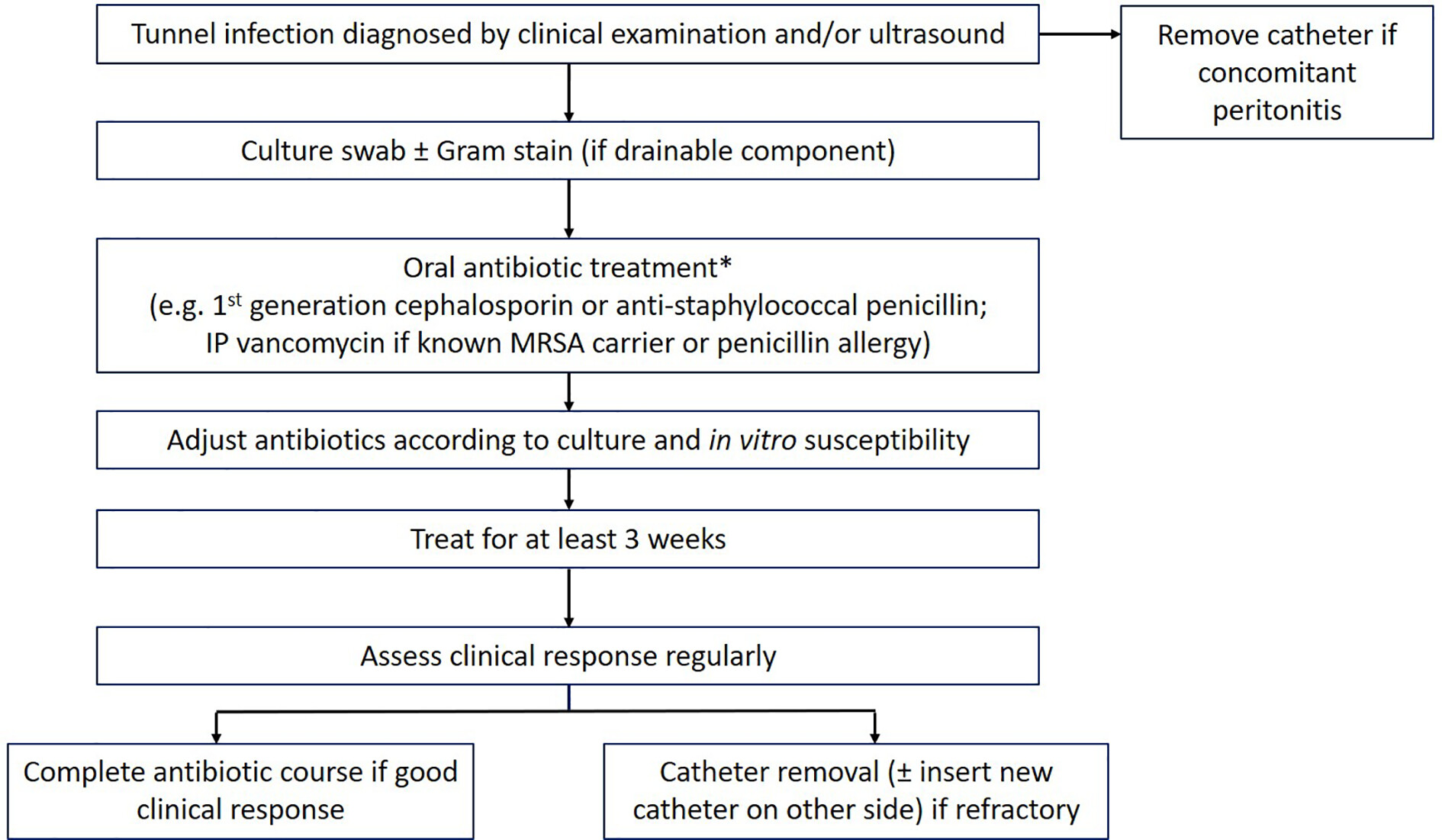
14 The 2022 Update of the ISPD Guidelines on Peritonitis Prevention and Treatment recommend ‘that systemic prophylactic antibiotics be administered immediately prior to catheter placement
(1A)’ in order to reduce the risk of catheter insertion-related peritonitis.
3 In a Cochrane systematic review and meta-analysis of antimicrobial agents for preventing infection in PD patients compared with placebo, pre- or peri-operative antibiotic prophylaxis had uncertain effects on catheter-related infection rates (4 studies, 379 participants; vancomycin risk ratio [RR] 0.36, 95% confidence interval [CI] 0.10–1.32, cefazolin RR 0.74, 95% CI 0.27–2.05, gentamicin RR 0.07, 95% CI 0–1.06, cefazolin + gentamicin RR 0.86, 95% CI 0.34–2.19, cefuroxime not estimable).
25 There are not sufficient data available to inform the preferred choice of IV antibiotics due to low methodological quality of studies conducted on this topic, although coverage of gram-positive organisms is likely important. No difference in catheter-related infection rate was observed between vancomycin 1000 mg IV administered 12 h before PD catheter insertion and cefazolin 1000 mg IV administered 3 h before PD catheter insertion (1 study, 178 participants: RR 0.49, 95% CI 0.13–1.89).
25,26 The use of nasal antibiotic prophylaxis had uncertain effects on the risk of exit site and tunnel infections (3 studies, 338 participants: RR 1.34, 95% CI 0.62–2.87), but there was evidence of a significant reduction in catheter-related infection among patients who were
S. aureus nasal carriers treated with mupirocin ointment (nasal application, twice daily for 5 days, every 4 weeks for up to 18 months; 1 study, 2626 patient-months: RR 0.57, 95% CI 0.39–0.84).
25 A systematic review and meta-analysis showed that mupirocin ointment treatment of
S. aureus nasal carriers was associated with a 74% lower probability of skin infection at the PD catheter exit site caused by
S. aureus compared with the control group (OR 0.26, 95% CI, 0.14–0.46).
27A systematic review of 17 RCTs reported no significant impact of different types of catheter placement techniques on preventing catheter-related infection. However, the number of studies examining the impact of insertion technique or placement on catheter-related infections was small with variable methodological quality at risk of imprecision. For example, laparoscopic insertion compared to laparotomy made little or no difference to the incidence of catheter-related infections (3 studies, 270 participants: RR 1.00, 95% CI 0.43–2.31,
p = 0.99). Similar results were observed for the subcutaneous burying or embedding of the PD catheter 6 weeks before initiation of PD (2 studies, 2511 patient-months: RR 1.15, 95% CI 0.39–3.42,
p = 0.8), midline versus lateral insertion of the PD catheter (2 studies, 120 participants: RR 0.56, 95% CI 0.12–2.58,
p = 0.45) and percutaneous insertion versus open surgical insertion (2 studies, 96 participants: RR 0.16, 95% CI 0.02–1.30,
p = 0.08).
28More recently, a systematic review and meta-analysis that included both observational (non-randomised) studies and RCTs found that, in low certainty evidence, percutaneous PD catheter insertion may have been associated with lower risks of early (within 1 month) exit site infection (7 studies; RR 0.36, 95% CI 0.24–0.53) and overall exit infection (16 studies; RR 0.61, 95% CI 0.46–0.82), but little or no difference in tunnel infection (7 studies; RR 0.76, 95% CI 0.38–1.51) compared with surgical (open and laparoscopic) PD catheter insertion.
29Prior to catheter insertion, it is advisable to carefully identify the optimal location of the exit site that will allow the patient to be able to see their exit site, clean it and avoid inadvertently traumatising it (e.g. by the belt).
14 An alternative peritoneal catheter exit site location (e.g. upper abdominal, pre-sternal) may be particularly important for patients with morbid obesity, intestinal stomas or urinary or faecal incontinence. Ideally, the location of the exit site should be chosen in advance of catheter insertion with the patient in the seated position. Preoperative mapping with sample catheters or a marking stencil may be helpful for choosing an appropriate catheter type. Following catheter insertion, in keeping with other post-surgical care, the insertion site is covered and left undisturbed to allow wound healing by primary intention.
14,30 The exit site dressing should best be left intact for 7 days unless soiled to immobilise the new catheter and reduce risk of infection.
14,30,31 Cytotoxic agents such as povidone-iodine or hydrogen peroxide are to be avoided till the sinus has healed.
30 In general, PD is recommended to start at least 2 weeks after catheter insertion.
14 Earlier commencement of PD has been shown to increase the risk of dialysate leak (1 study, 122 participants: RR 3.90, 95% CI 1.56–9.78) with uncertain effect on the risk of exit site infection (2 cohort studies, 337 participants: RR 1.43, 95% CI 0.24–8.61; 1 case–control study, 104 participants: RR 1.20, 95% CI 0.41–3.50).
32Exit site care
•
We recommend daily topical application of antibiotic cream or ointment (mupirocin or gentamicin) to the catheter exit site to prevent catheter-related infection (1C).
•
We suggest that the comparative efficacies of topical mupirocin versus topical gentamicin or exit site versus nasal application of mupirocin for preventing catheter-related infection are uncertain (2C).
•
We suggest that no cleansing agent has been shown to be superior to any other with respect to preventing catheter-related infections (2B).
•
We recommend that the exit site be cleansed at least twice weekly and every time after a shower or vigorous exercise, including running, cycling, swimming and water sports (1C).
•
We recommend that PD catheter exit site care be continued after interruption or discontinuation of PD for as long as the catheter remains in place (Not Graded).
•
We suggest that a dressing cover over the exit site is not mandatory after exit site care and topical antibiotic application (2D).
•
We recommend that the PD catheter be immobilised to avoid traction injury of the exit site (1C).
Daily application of mupirocin to the exit site has been shown to be a cost-effective strategy to decrease the risk of exit site infection from
S. aureus, in observational studies, RCTs and meta-analyses.
45–47 Application of mupirocin was reported to reduce the risk of exit site infections by 62% among patients undergoing PD (five studies: RR 0.38, 95% CI 0.22–0.67).
46 In this systematic review, three studies involved nasal mupirocin application and two involved exit site application. Indeed, the site, frequency and duration of mupirocin treatment have been highly variable across the studies conducted to date thereby limiting their ability to inform standardised practice.
48 Daily administration is not as likely to induce mupirocin resistance compared with intermittent dosing, but the long-term implication remains uncertain.
49,50 A Cochrane systematic review and meta-analysis reported that topical nasal application of mupirocin had uncertain effects on exit site infection (3 studies, 338 participants: RR 1.34, 95% CI 0.62–2.87).
25 Unfortunately, exit site application of mupirocin was grouped with oral antibiotic prophylaxis (floxacin, cephalexin, rifampin or cotrimoxazole). While the overall analysis showed an uncertain effect of oral or topical antimicrobial prophylaxis on exit site infection (5 studies, 395 participants: RR 0.82, 95% CI 0.57–1.19) with moderate heterogeneity (
I 2 = 40%,
p = 0.17), the specific effect of topical exit site mupirocin was not evaluated. Obata and colleagues have recently completed an updated systematic review and meta-analysis of RCTs (six studies), examining topical exit site application of mupirocin compared to other exit site care interventions.
51 In contrast to previous findings of superior benefit compared to standard care, their systematic review demonstrated that it was uncertain whether the application of mupirocin ointment prevents exit site infection (RR 0.36, 95% CI 0.13–1.05). This analysis is limited by the moderately high level of heterogeneity (
I 2 = 61%,
p = 0.07) between the studies.
51 In summary, the available evidence from systematic reviews and meta-analyses of RCTs suggest that topical mupirocin prophylaxis may reduce the risk of catheter-related infections. However, the certainty of this evidence is reduced by indirectness (highly variable approaches to administering the intervention including nasal vs. exit site application), risk of bias and inconsistency. There is also a lack of direct comparison between nasal and exit site application of mupirocin with respect to risk of catheter-related infection. For these reasons, the Guideline Working Group downgraded the strength of the topical mupirocin prophylaxis recommendation from 1A in the 2017 Guidelines to 1C currently. It also was not able to recommend the optimal site of topical application (nasal vs. exit site). Currently, there is a multi-centre, double-blind RCT underway in Thailand (COSMO-PD Trial) examining the comparative effectiveness of local application of chlorhexidine gluconate, mupirocin ointment and normal saline for prevention of PD-related infections.
52 Hopefully, the results from this trial will help guide future recommendations on this topic.
An alternative topical antibacterial prophylactic agent is gentamicin. Daily application of gentamicin to the exit site was shown to be highly effective in preventing exit site infection caused by
Pseudomonas species, and as effective as topical mupirocin in reducing
S. aureus exit site infections in a three centre, double-blind RCT (
n = 133).
13 However, its broad implementation has been restricted by limited availability and concerns of a change in the microbiologic profile of organisms responsible for catheter-related infection, gentamicin resistance
53,54 and development of other atypical infections.
55 Alternating between mupirocin and gentamicin exit site application has been discouraged due to observed increase in the risk of fungal peritonitis compared with gentamicin alone.
56 A recent systematic review and meta-analysis observed no difference in the rate of exit site infection between topical exit site application of mupirocin or gentamicin (2 studies, 228 participants: RR 1.14, 95% CI 0.27–4.81) with high heterogeneity (
I 2 = 87%,
p = 0.005).
51Other prophylactic strategies examined include the use of medical-grade antibacterial honey at the exit site, which has been shown to have a similar risk of catheter-related infections to that of patients treated with intranasal mupirocin appointment (incidence rate ratio [IRR] 1.12, 95% CI 0.81–1.53).
57 More importantly, exit site application of honey increased the risk of catheter-related infection and peritonitis among patients with diabetes, thereby precluding its use in this subgroup.
22 There are several other studies showing mixed results pertaining to the use of topical polysporin triple ointment,
58 topical polyhexanide
59 and polyhexamethylene biguanide
60 and nanotechnology antimicrobial spray dressing
61 to prevent exit site infections. Further studies on these agents are required prior to consideration for their broad use in clinical settings.
It should also be noted that contact between ointments/creams and the PD catheter should be minimised as there have been reports that the polyethylene glycol base in mupirocin can damage polyurethane catheters and that gentamicin cream may damage silicone catheters.
62–64A PDOPPS study of infection prevention strategies by 170 centres caring for 11,389 patients in 7 countries reported wide variation in exit site cleaning strategies, including antibacterial soap, non-antibacterial soap, chlorhexidine, povidone-iodine, sodium hypochlorite and other agents.
17 Antibacterial soap was used to clean the catheter exit sites in 57% of US, 40% of Canadian and 39% of Australian and New Zealand units.
17 There have been studies comparing its effectiveness against other topical cleaning agents, with varying results. Povidone-iodine, also known as iodopovidone, is an antiseptic commonly used for skin disinfection before and after surgery. Its effectiveness compared to soap and water or no specific care in reducing the incidence of catheter-related infection has been inconsistently demonstrated. For example, in an RCT including 127 patients from 8 hospitals, participants receiving povidone-iodine had a significantly lower occurrence of exit site infection compared to those using soap and water (0.27 episodes/patient-year vs. 0.71 episodes/patient-year).
65 However, similar results have not been observed by others.
66 Moreover, there have been concerns regarding the risk of irritation induced by the regular application of povidone-iodine precipitating secondary exit site infection.
67 Similar concerns of local irritability have been raised for chlorhexidine gluconate (0.05–2% aqueous solution with or without isopropyl alcohol with broad-spectrum antimicrobial activities). As an alternative, chlorhexidine-impregnated sponge dressing has been developed allowing weekly application. A single-centre pilot study of 50 incident PD patients from Singapore using chlorhexidine-impregnated sponge demonstrated low catheter-related infection rates (0.09 episodes/patient-year, 95% CI 0.02–0.22) with 92% 1-year infection-free survival. Although 73% of participants reported these dressings to be acceptable, 12% developed localised contact dermatitis.
68 The outcomes from this study should be interpreted with caution due to the lack of concurrent comparison group and small sample size, warranting further studies to be conducted prior to broader implementation. Another cleansing agent, Amuchina solution, an electrolytic chloroxidizing solution containing sodium hypochlorite (3–10%), has been shown to be effective in preventing exit site infection in paediatric patients
69 without any secondary skin reaction. A retrospective observational study of 83 paediatric PD patients observed a significant reduction in catheter-related infection rates from 1.36 episodes per patient-year with application of mupirocin at exit site to 0.33 episodes per patient-year when mupirocin was augmented with sodium hypochlorite solution (
p < 0.0001) without occurrence of mupirocin-resistant organisms.
70 However, these findings should be interpreted carefully due to the limitations of study sample size and design. There have also been inconsistent outcomes among studies in which head-to-head comparisons of different types of disinfectants (i.e. povidone-iodine, chlorhexidine, hypochlorite) were performed to inform clinical decision-making.
71,72 A Cochrane systematic review and meta-analysis reported very low certainty evidence that various dressing systems (chlorhexidine, povidone-iodine, sodium hypochlorite gauze + fixomull, blister film) may make little or no difference to exit site infection rates.
25 New topical antiseptic such as polyhexanide had also been tested, albeit in an underpowered study.
73In addition to the therapeutic benefit of dressing or antiseptic agents, we should be cautious about contaminated products, especially when they are not considered to be pharmaceutical products. Suboptimal manufacturing practice or preparation could have been the cause of contaminated aqueous chlorhexidine solution,
74–76 leading to several
Burkholderia cepacia complex PD catheter exit site infection outbreaks, as reported in New Zealand
77 and Hong Kong.
74The optimal frequency of exit site care has not been tested by RCTs. However, exit site care frequency less than twice weekly appeared to be associated with higher odds of catheter-related infections.
78 Exit site care is therefore recommended at least twice weekly, and every time after water contamination or vigorous exercise, to keep clean and dry.
79 Preliminary data suggested avoidance of water exposure to prevent introduction of water-derived organisms. In a small single-centre observational (non-randomised) study, application of a stoma bag during the daily shower was associated with reduction of exit site infection.
80 However, this evidence was very low certainty. Covering the exit site during swimming has also been recommended by the 2022 ISPD Guidelines on Physical Activity and Exercise in Peritoneal Dialysis to protect the exit site from getting wet.
79 These guidelines further suggest that ‘swimming or other water sports should preferably take place in either sea water or swimming pools that are known to be well maintained (private or municipal) to limit exposure to waterborne pathogens. (2D)’
79 The evidence underpinning this guideline is very low certainty based on anecdotal experience.
Although previous ISPD guidelines have not addressed the care of exit site after PD discontinuation (in the setting of catheter dysfunction, hernia complication or waiting for catheter removal after kidney transplantation or transfer to haemodialysis), we recommend similar intensity or frequency of exit site care. The patient should be given information about the need to cleanse and monitor the exit site even after PD interruption or discontinuation.
Contrary to the previous recommendation to protect the exit site with dressing material such as sterile gauze coverage, continuing this practice beyond the immediate post-operative period is not supported by one RCT
18 and two observational studies.
78,81 A single-centre, open-label RCT involving 97 participants in Malaysia showed that simple washing and cleansing of the exit site followed by topical mupirocin with or without a dressing cover resulted in similar incidences of catheter-related infection.
18 The exceptionally low exit site infection rate in this study, at 0.05–0.11 episodes per year, could have limited the external validity of their findings. Rates of exit site infection were also not associated with application of dressings according to a multi-centre cross-sectional survey of 1204 patients from 12 PD centres in China.
78 Another retrospective study showed that routine dressing of the exit site (
n = 54) was associated with higher exit site infection rate than in the non-dressing group (
n = 12).
81 Transparent or semi-occlusive dressing material did not appear to be associated with exit site infection rates in 2460 participants in the BRAZPD II study.
82 Taken together, current evidence is not sufficient to support the use of covered dressings. Furthermore, concerns have been raised about the potential for covered dressings to cause local allergic reactions and acceleration of local bacterial growth. This information needs to be balanced against other considerations with respect to dressings, such as mitigating exposure to environmental dusts and animal danders, avoiding staining of clothing by topical antimicrobial ointment, providing extra padding and facilitating catheter immobilisation.
While there is insufficient evidence to support covering the exit site, fixing or immobilising the catheter in place is recommended to prevent traction of or frictional injury to the exit site. The practice of fixing the catheter by waist belt, protective bag or securing the transfer/extension set to the abdomen by adhesive tape is supported by several observational studies on risk factors of exit site infection. A history of catheter pulling injury or traction bleeding, based on multivariate regression analysis, was associated with increased exit site infections in two studies (hazard ratio 1.78, 95% CI 1.02–3.11
19 and 2.44, 95% CI 1.47–4.04
78). We believe this recommendation of fixing the PD catheter also aligns with the ISPD and the Global Renal Exercise Network practice recommendations
79 to avoid repetitive rubbing of the catheter site during sports activity, and the use of a belt during sports to provide protection.