

Occupational noise-induced hearing loss: What is the contribution of personal noise exposures? A case study of mineworkers at a large-scale platinum mine in South Africa
Abstract
Introduction
Methods
Study design and data collection
Data analysis
| Characteristic | All | ≤25 normal | STS change (dBHL) | p Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 26-45 mild | 46–55 moderate | 56–70 Moderately severe | 71 + severe | ||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||
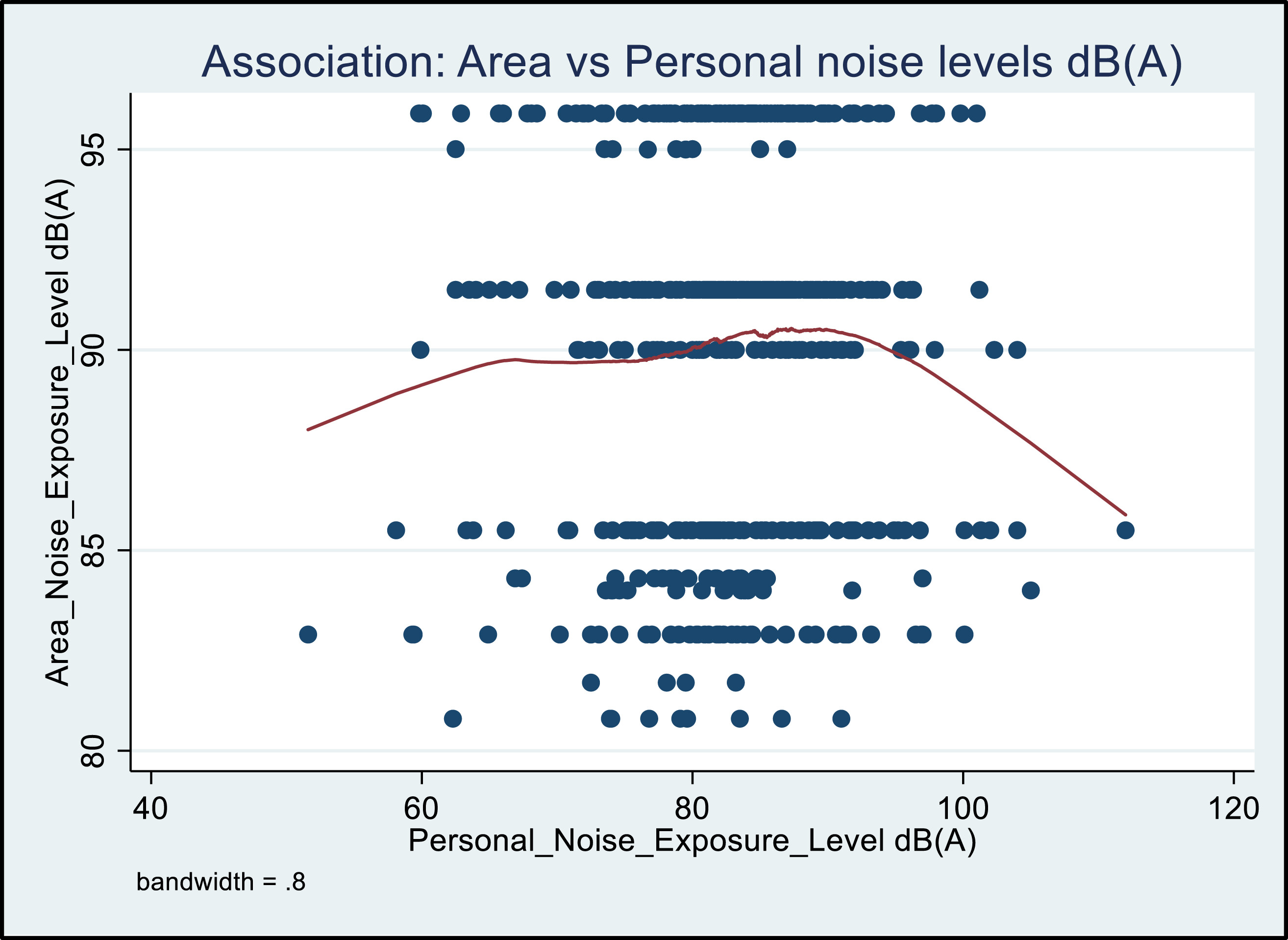
| Personal noise dB(A) | |||||||||||||
| ≤81.99-84.99 | 313 | 60.1 | 260 | 49.9 | 38 | 7.3 | 7 | 1.3 | 4 | 0.8 | 4 | 0.6 | 0.910 |
| ≥85-105 | 208 | 39.9 | 176 | 33.8 | 27 | 5.2 | 4 | 0.8 | 1 | 0.2 | 0 | 0.0 | |
| Age (years) | |||||||||||||
| ≤25 | 3 | 0.6 | 3 | 0.6 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0.000 |
| 26-40 | 209 | 40.1 | 203 | 39.9 | 3 | 0.6 | 0 | 0.0 | 2 | 0.4 | 1 | 0.2 | |
| 41-55 | 242 | 46.4 | 199 | 38.1 | 34 | 6.5 | 5 | 1.0 | 2 | 0.4 | 2 | 0.4 | |
| 56-65 | 67 | 12.9 | 31 | 6.0 | 28 | 5.4 | 6 | 1.2 | 1 | 0.2 | 1 | 0.2 | |
| Sex | |||||||||||||
| Male | 480 | 92.1 | 397 | 76.2 | 64 | 12.3 | 11 | 2.1 | 4 | 0.8 | 4 | 0.8 | 0.160 |
| Female | 41 | 7.9 | 39 | 7.5 | 1 | 0.2 | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | |
| Shift (hours) | |||||||||||||
| ≤8 | 76 | 14.6 | 66 | 12.7 | 8 | 1.5 | 1 | 0.2 | 0 | 0.0 | 1 | 0.2 | 0.764 |
| >8 | 445 | 85.4 | 370 | 70.0 | 57 | 10.9 | 10 | 1.9 | 5 | 1.0 | 3 | 0.6 | |
| Total | 521 | 100 | 436 | 83.7 | 65 | 12.5 | 11 | 2.11 | 5 | 1.0 | 4 | 0.8 | |
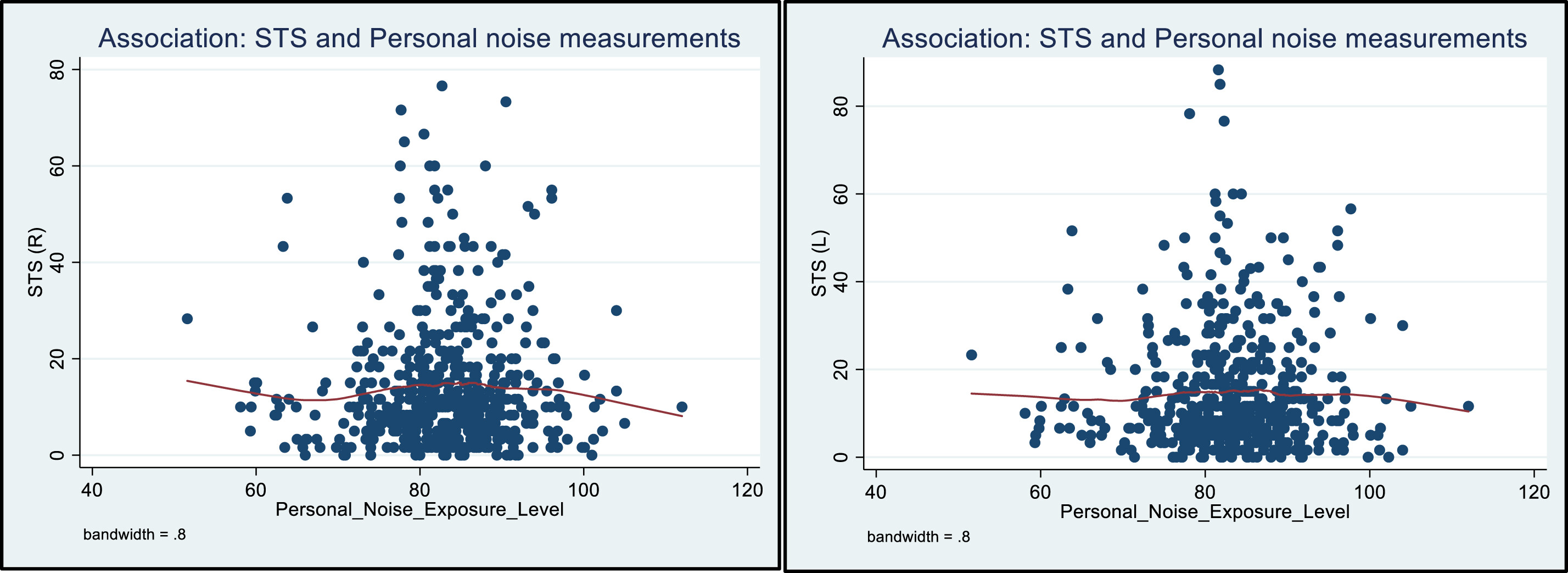
| Associations between variables and STS changes (Right ear) | |||||||||||||
| Personal noise exposure dB(A) | |||||||||||||
| ≤81.99-84.99 | 313 | 60.1 | 266 | 51.1 | 32 | 6.1 | 8 | 1.5 | 5 | 1.0 | 2 | 0.4 | 0.834 |
| ≥85-105 | 208 | 39.9 | 174 | 33.4 | 28 | 5.4 | 4 | 0.8 | 1 | 0.2 | 1 | 0.2 | |
| Age (years) | |||||||||||||
| ≤25 | 3 | 0.6 | 3 | 0.6 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0.000 |
| 26-40 | 209 | 40.1 | 201 | 38.6 | 6 | 1.2 | 1 | 0.2 | 1 | 0.2 | 0 | 0.0 | |
| 41-55 | 242 | 46.4 | 201 | 38.6 | 33 | 6.3 | 5 | 1.0 | 1 | 0.2 | 2 | 0.4 | |
| 56-65 | 67 | 12.9 | 35 | 6.7 | 21 | 4.0 | 6 | 1.2 | 4 | 0.8 | 1 | 0.2 | |
| Sex | |||||||||||||
| Male | 480 | 92.1 | 402 | 77.2 | 57 | 10.9 | 12 | 2.3 | 6 | 1.2 | 3 | 0.6 | 0.586 |
| Female | 41 | 7.9 | 38 | 7.3 | 3 | 0.6 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Shift duration (hours) | |||||||||||||
| ≤8 | 76 | 14.6 | 65 | 12.8 | 8 | 1.5 | 3 | 0.6 | 0 | 0.0 | 0 | 0.0 | 0.615 |
| >8.1 | 445 | 85.4 | 375 | 72.0 | 52 | 10.0 | 9 | 1.7 | 6 | 1.2 | 3 | 0.6 | |
| Total | 521 | 100 | 440 | 84.5 | 60 | 11.5 | 12 | 2.3 | 6 | 1.2 | 3 | 0.6 | |
Results
| Hearing deterioration (STS)/Variables | *RRR | 95% CI | p Value | |||
|---|---|---|---|---|---|---|
| Left ear | Right ear | Left ear | Right ear | Left ear | Right ear | |
| Mild | ||||||
| Age | 6.734 | 4.412 | 4.180-10.849 | 2.818-6.907 | <0.001 | <0.001 |
| Personal noise | 1.156 | 1.319 | 0.841 -1.588 | 0. 959-1.814 | 0.370 | 0.088 |
| Shift duration | 1.063 | 0.910 | 0.449-2.514 | 0.393- 2.106 | 0.890 | 0.827 |
| Moderate | ||||||
| Age | 10.213 | 6.754 | 3.442-30.296 | 2.576-17.707 | <0.001 | <0.001 |
| Personal noise | 0. 910 | 1.081 | 0. 458-1.807 | 0.564-2.073 | 0.788 | 0.813 |
| Shift duration | 1.508 | 0. 420 | 0.180-12.640 | 0.104-1.698 | 0.705 | 0.224 |
| Moderate-severe | ||||||
| Age | 1.566 | 6.815 | −0.874-1.835 | 1.705-27.236 | 0.487 | 0.007 |
| Personal noise | 0.756 | 0. 423 | −1.225-0.779 | 0.125-1.427 | 0.587 | 0.166 |
| Shift duration | 0 | 0 | 0 | 0 | 0.979 | 0.987 |
| Severe | ||||||
| Age | 2.386 | 5.047 | 0.528-10.770 | 0.844-30.182 | 0.258 | 0.076 |
| Personal noise | 0.315 | 1.087 | 0.056-1.774 | 0.312-3.786 | 0.191 | 0.895 |
| Shift duration | 0.628 | 0 | 0. 062-6.286 | 0 | 0.692 | 0.992 |
Discussion
Risk-based audiometry assessment
Assessment outcomes of risk-based audiometry medical surveillance
Conclusion
Acknowledgments
Ethical approval
Consent for publication
Declaration of conflicting interests
Funding
ORCID iDs
Footnote
References
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In
Keywords
Rights and permissions
Article versions
Authors
Metrics and citations
Metrics
Journals metrics
This article was published in Noise & Vibration Worldwide.
View All Journal MetricsPublication usage*
Total views and downloads: 466
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 0
Crossref:
There are no citing articles to show.
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
IOM3 members can access this journal content using society membership credentials.
IOM3 members can access this journal content using society membership credentials.
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.
