

Parental Decision-Making Around Introducing Complementary Foods: An Integrative Review
Abstract
Introduction
Feeding: A Parenting Role
Parenting Through Feeding Transitions
Current CF Recommendations
Existing Work
Guiding Framework
Aims
Methods
Eligibility Criteria
Information Sources and Search Strategy
Study Selection
Risk of Bias Assessment
Data Extraction and Data Synthesis


Results
Study Characteristics

| Author (year) | Study type | Adult participant (Special study population; geography) | Data source | Study design Infant age | % of age-appropriate introduction | Factors associated with age of introduction | Factors not associated with age of introduction | Information sources |
|---|---|---|---|---|---|---|---|---|
| Barrera et al. (2018) | QUANT | Any caregiver (Nationally representative) | 2009-2014 continuous National Health and Nutrition Examination Survey | CROSS 6-36 mo | 37.2% between 6 and 8 mo | After adjusting for covariates, infants who were never breastfed or breastfed <4 mo were more likely to be introduced to CF early. | After adjusting for covariates, infant race and ethnicity, WIC receipt, and maternal age were not significant. | |
| Clayton et al. (2013) | QUANT | Mother (Nationally representative) | IFPSII | LONG Monthly from birth to 12 mo | 7.1% at >6 mo | Breastfed infants introduced later than formula and mixed-feeding infants. Mothers who introduced early were more likely to be younger, unmarried, have lower educational attainment, lower income, and participate in WIC. | Endorsing that their baby was old enough or baby wanted the food they ate. | 55% of mothers who introduced before 4 mo did so because a physician or health care professional told them to. |
| Doub et al. (2015) | QUANT | Mother (No specific sampling; central PA) | Independent sample | LONG 4 and 6 mo | 12.7% at or after 6 mo | Mothers who introduced on time more likely to be older, have higher educational attainment, leaner, and pay more attention to their infants’ hunger and fullness cues. | Infant sex, birthweight, birth order, formula vs. mixed feeding. | |
| Kim and Gallien (2016) | QUANT | Parent or guardian (Nationally representative) | 2007 National Survey of Children’s Health | CROSS 0-24 mo | NR | Infants of single mothers were more likely to be introduced to CF before 4 mo compared with infants from two parent households, but this was not statistically significant. | ||
| Mehta et al. (2012) | QUANT | Mother (No specific sampling; North Carolina) | Pregnancy, Infection and Nutrition Study, postpartum | LONG 3 and 12 mo | 75.3% between 4 and 6 mo; 5.1% after 6 mo | Introduction before 4 mo was associated with mothers who were non-White race, overweight/obese before pregnancy, multiparous, unmarried, had lower educational attainment, and lower income, were less likely to have initiated or breastfed to 3 mo, had higher levels of depression, stress, and anxiety symptoms during pregnancy. | Psychological factors were no longer associated with early introduction once race, education, and poverty level were included in the model. | |
| Roess et al. (2018) | QUANT | All caregivers (Nationally representative) | Feeding Infants and Toddlers Study | CROSS 0-23.9 mo | 73% between 4 and 5.9 mo | Formula consumption: Among 0 to 3.9 mo olds, 27% of those receiving formula ate CF vs. 5% of infants not receiving formula. Among 4 to 5.9 mo olds, 85% of those receiving formula ate CF vs. 51% of infants not receiving formula. | ||
| Sanjeevi et al. (2022) | QUANT | Mother (No specific sampling; North Carolina) | Pregnancy Eating Attributes Study | LONG 6, 9, and 12 mo | Mean 4.9 mo | Greater infant enjoyment of food was associated with 65% lower odds of early introduction (before 4 mo; not statistically significant) and higher age of introduction (statistically significant). | Infant food responsiveness, satiety responsiveness, slowness in eating, and overall appetite were not associated with age of introduction. |
| Author (year) | Study type | Adult participant (special study population; geography) | Data source | Study design Infant age | % of age-appropriate introduction | Factors associated with age of introduction | Factors not associated with age of introduction | Information sources |
|---|---|---|---|---|---|---|---|---|
| Braid et al. (2015) | QUANT | Mother (Term vs. preterm; nationally Representative) | Early Childhood Longitudinal Study | CROSS 9 mo | 72.3% at or greater than 4 mo | Analyzed together: Early introduction in term and preterm infants who: had mothers who were under 30 years, current smokers, never breastfed or breastfed <1 mo, lower SES, entered daycare earlier. Lower risk of early introduction among Asian infants. Preterm infants born to underweight mothers had lower odds of early introduction; those to younger mothers had early introduction. Preterm were more likely to be introduced early than term infants. | ||
| Cochran et al. (2022) | MIXED | Mother (Parent of infant with Down syndrome; Pacific Northwest) | Independent sample | CROSS 12-60 mo | 52.17% at 6-8 mo Mean for infants with DS: 6.2 mo (SD: 2.0) Mean for siblings: 5.1 mo (SD: 1.3) | Infants with DS introduced later than siblings, based on observed signs of readiness (or not being ready earlier) and caution due to medical complications of DS. Some families based age of introduction on their experience with their other children. | 32% of parents were not given specific advice on age of introduction. 69% of parents who received advice got it from their PCP while 31% received it from other sources (i.e., feeding clinic). | |
| Gaffney et al. (2014) | QUANT | Mother (PPD vs. no PPD; national distribution) | IFPSII | LONG Monthly from birth to 12 mo | 73% at >4 mo | PPD when adjusted for potential confounders. Mother’s race, age, household income, pre-pregnancy BMI, postpartum smoking status. Infant sex, fussiness as a problem. | ||
| Hoffman et al. (2014) | QUANT | Mother (ED vs. no ED; North Carolina) | Independent sample | CROSS 6-36 mo | 80-96% at 4-6 mo | Eating disorder hx vs. none; nonsignificant trend toward more infants of mothers with hx of ED being introduced to solid foods after 7 mo. | ||
| Khalessi and Reich (2013) | QUANT | Mother (Primiparous; Southern United States) | Baby Books Project | LONG 2, 4, 6, 9, 12, and 18 mo | NR | Women who breastfed were more likely to delay the introduction to CF. African American mothers were more likely to introduce CF early. | ||
| McKean et al. (2015) | QUANT | Mother; father; guardian (At least one parent with hx of asthma; San Francisco Bay area) | Trial of Infant Probiotic Supplementation | LONG Prenatal, at birth, monthly 0-12 mo, every 6 mo, 12-36 mo | 13.4% at 6 mo | Late introduction was associated with maternal history of food allergy dx and Asian race. | ||
| Michels et al. (2016) | QUANT | Mother (Conceived with vs. without fertility treatment; New York) | Upstate KIDS | LONG 4, 8, and 12 mo | NR | Mothers who conceived with fertility treatments were slightly less likely to introduce CF at 4 mo and more likely to have introduced by 8 mo; however, when adjusted for daycare initiation and timely completion of the questionnaire, mothers who used fertility tx were at higher risk for early introduction of CF. | ||
| Thullen et al. (2016) | QUAL | Mother; father (Co-parenting parents; rural Midwest United States) | Independent sample | CROSS 6-36 mo | NR | Parents looked for cues, read information, and received advice from friends. At the transition to CF, fathers became more involved in feeding and feeding decisions. |
| Author (year) | Study type | Adult participant (Special study population; geography) | Data source | Study design Infant age | % of age-appropriate introduction | Factors associated with age of introduction | Factors not associated with age of introduction | Information sources |
|---|---|---|---|---|---|---|---|---|
| DiSantis et al. (2013) | QUANT | Mother (Equal representation of Hispanic, black, and white identifying; Houston area) | Fisher et al., 2008 | CROSS 7-24 mo | Infants who were breastfed <3 mo or 3-6 mo received CF earlier than those breastfed more than 6 mo. | |||
| Hartman et al. (2016) | QUANT | Any caregiver (Suburban insurance vs. urban Medicaid; Cincinnati, OH area) | Independent sample | CROSS 4-36 mo | Mean for urban population: 4.74 mo (SD: 1.49) Mean for suburban population: 5.1 mo (SD: 1.14) | Recommended age for introduction was most influential in parent decision but was not statistically significant. | No difference in age of introduction between the urban and suburban groups. Recommended age, maternal education, race, maternal age, insurance type, number of children, and allergy risk were not significant influences on timing of introduction. | Recommended age for CF introduction by the infant’s health care professional was the most important variable. |
| Horodynski and Mills (2014) | QUAL | Mother (Low-income adolescents; Michigan) | Independent sample | CROSS 0-12 mo | NR | Mothers who introduced early had the perception that breast milk/formula alone was not sufficient to fill their babies up (lacked knowledge of how much formula or breast milk their babies needed). Someone else (e.g., friends, family) would feed baby CF before 4 mo. | Advice from own mother was most impactful. Varying adherence to advice of health care professionals. Conflicting advice received from friends/family vs. health professionals. | |
| Hurley et al. (2015) | QUANT | Mother (WIC participants; Maryland) | Maryland Infant Feeding Study | CROSS 0-12 mo | 84.2% between 4 and 6 mo | Mothers who added cereal to their infant’s bottle were more likely to introduce CF before 4 mo. Greater maternal stress associated with introducing CF before 4 mo. | ||
| Johnson et al. (2019) | QUAL | Mother and a caregiver (Marshallese; Arkansas) | Independent sample | CROSS 0-36 mo | M: 10.2 mo | Infant’s interest in eating was the main influence for introducing CF. Mothers who introduced early had the perception that milk/formula alone was not sufficient for infant development. Mothers who introduced late waited until infants had teeth and could chew. | Caregivers are responsible for making mealtime decisions and preparing meals. Caregivers provide support and advice to mothers. | |
| Kim and Mathai (2015) | QUANT | Any caregiver (In WIC with PC or CC; Central Illinois) | Caretaker Research Advancing Youth Obesity and kNowledge | CROSS 2-8 mo | Mean 4.28 mo for PC; 4.51 for CC | Infants in CC vs. PC, but neither met AAP infant feeding recommendations. | ||
| Lee and Brann (2015) | QUAL | Mother (Chinese American; New York City) | CROSS 0-12 mo | Some | Mothers introduce CF early due to the perceived benefits for the infant: strengthening bone development, prolonging satiety, accelerating growth, improving digestion, and preparing/teaching how to swallow adult foods. | |||
| Lindsay et al. (2017) | QUAL | Mother (Brazilian immigrants; greater Boston, MA) | Independent sample | CROSS 24-60 mo | Most introduced around 4 mo | Mothers introduced CF early due to cues of infant hunger and lack of satiety. | Their own mother’s and relatives’ infant feeding practices influenced their own practices. Advice from health care providers often conflicted with cultural beliefs and practices. Mothers felt more comfortable following advice of own mothers/friends even when it was counter to health care providers’ advice. WIC was an important source of information. | |
| McFarren et al. (2020) | QUAL | Mother; foster mother (Latinx; Central Texas) | Independent sample | CROSS 6-18 mo | NR | CF are introduced earlier in their home countries (Mexico/Central America). | Pediatrician and WIC were common sources of information. | |
| McManus et al. (2017) | QUANT | Mother (Ethnically diverse, low income, primiparous; Southern United States) | Baby Books Project | LONG Prenatal, 2, 4, 6, 9, 12, and 18 mo | 70% between 6 and 8 mo | Women who felt more “uplifts” compared with “hassles” during pregnancy were more likely to have better overall nutritional practices with their infant, including age-appropriate introduction to CF. | ||
| Vadiveloo et al. (2019) | QUANT | Mother (Predominantly non-Hispanic Black; Durham, NC) | Nurture Study | LONG Birth to 12 mo, every 3 mo | NR | Primary factor for early introduction was that baby seemed hungry (68.3%). Other factors were: baby was drinking too much formula (51.2%), belief solids would help baby sleep (48.8%), baby was old enough to begin solids (48.8%), and baby was showing an interest in solids (45.7%). Significant interaction between maternal pre-pregnancy BMI and early introduction. | ||
| Vandyousefi et al.(2022) | QUANT | Mother (low-income Hispanic; New York City) | Starting Early Program | LONG 3, 10, 19, 24, and 36 mo | NR | Infants with higher slowness in eating and satiety responsiveness scores were less likely to be introduced to CF early. | Food responsiveness and enjoyment of food were not significantly related to age of introduction. | |
| Wasser et al. (2013) | QUANT | Mother (low income, primiparous, African American; North Carolina) | Infant Care, Feeding and Risk of Obesity Study | LONG 3, 6, 9, 12, and18 mo | NR | No association between use of a non-maternal caregiver and early introduction to CF. | Fathers were more involved with feeding if they were married and may be more involved in feeding early in infancy. Grandmothers were less likely to be involved with feeding in married households and if the mother was older. | |
| Woo Baidal et al. (2015) | QUAL | Mother (Hispanic; eastern Massachusetts) | Independent sample | CROSS 0-24 mo | NR | Mothers introduced early based on the belief that adding solids to bottles helped infants feel full, gain more weight, calm down, and receive adequate nutrition. Family beliefs that infants need a variety of foods to develop taste preferences led to early introduction. Relatives wanted to feed infant CF early. | Female family members were common sources of information. Mothers wanted more easily accessible information from pediatrician. |
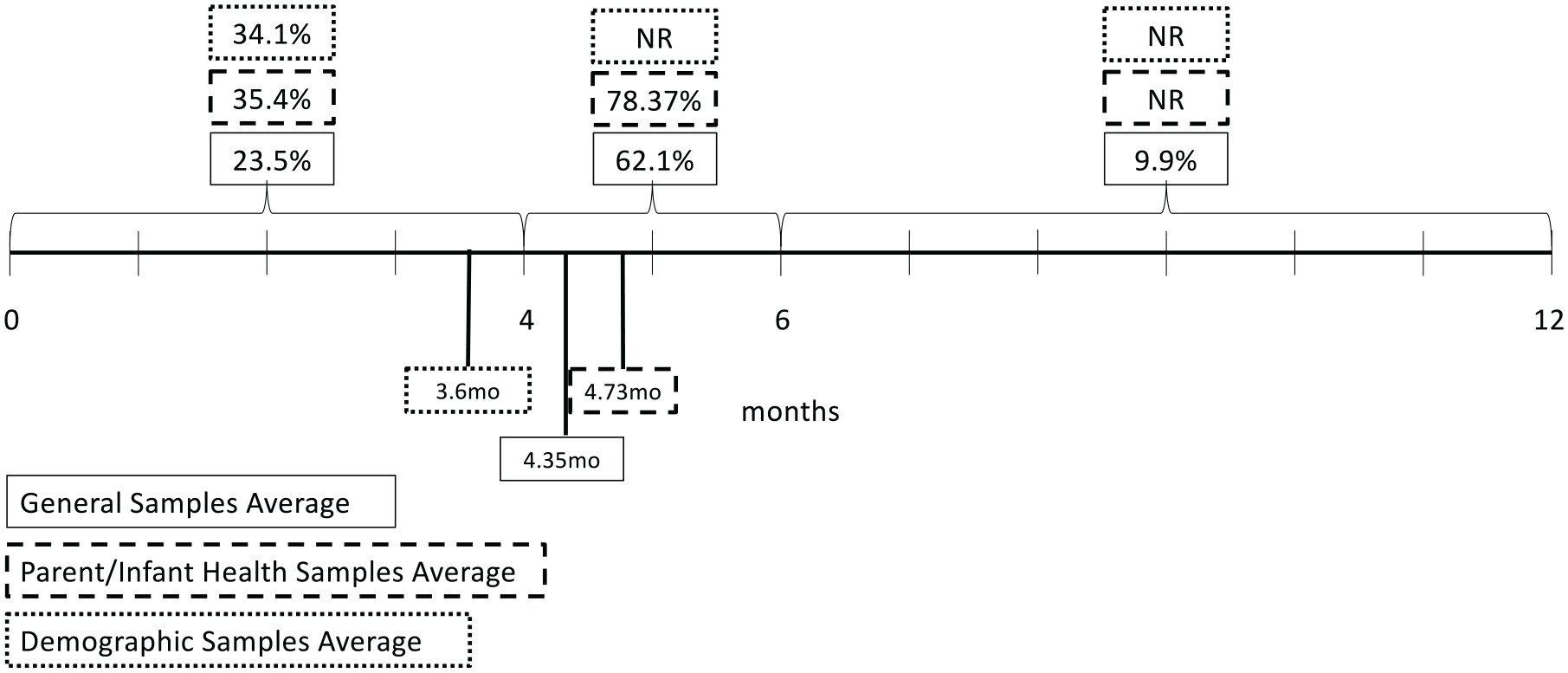
Age of Introduction to CF
| Author (year) | Definition of “Early introduction” | Definition of appropriate age of introduction |
|---|---|---|
| Barrera et al. (2018) | Before 4 months | Debated, 4-6 months or 6 months |
| Braid et al. (2015) | Before 4 months | Debated, 4-6 months or 6 months |
| Clayton et al. (2013) | Before 4 months | About 6 months |
| Cochran et al. (2022) | Not specified | 6 months |
| DiSantis et al. (2013) | Not specified | Not specified |
| Doub et al. (2015) | Before 4 months | Changing guidelines: 4-6 months and 6 months |
| Gaffney et al. (2014) | Not specified | Not specified |
| Hartman et al. (2016) | Not specified | 4-6 months |
| Hoffman et al. (2014) | Not specified | 4-6 months |
| Horodynski & Mills (2014) | Before 4 months | 4-6 months |
| Hurley et al. (2012) | Before 4 months | 6 months |
| Johnson et al. (2019) | Before 6 months | After 6 months |
| Khalessi & Reich (2013) | Before 4 months | 4-6 months |
| Kim & Mathai (2015) | Not specified | After 6 months |
| Kim & Gallien (2016) | Before 4 months | 4-6 months |
| Lee & Brann (2015) | Before 6 months | Not specified |
| Lindsay et al. (2017) | Not specified | 6 months |
| McFarren et al. (2020) | Not specified | Not specified |
| McKean et al. (2015) | None | Debated, 4-6 months |
| McManus et al. (2017) | Before 4 months | 4-6 months |
| Mehta et al. (2012) | Before 4 months | After 4 months, preferably 6 months |
| Michels et al. (2016) | Not specified | 6 months |
| Roess et al. (2018) | Before 4 months | 4-6 months |
| Sanjeevi et al. (2022) | Before 4 months | Debated, 4-6 months or 6 months |
| Thullen et al. (2016) | Not specified | Approximately 6 months |
| Vadiveloo et al. (2020) | Before 4 months | Not specified |
| Vandyousefi et al. (2022) | Before 4 months | 6 months |
| Wasser et al. (2013) | Before 4 months | 6 months |
| Woo Baidal et al. (2015) | Before 4 months | 4-6 months |
Factors That Influence Age of Introduction
Individual level
Demographics
Maternal behaviors
Maternal beliefs and perceptions
Maternal mental health
Interpersonal level
Community level
Societal level
Information Sources
Recommendations for Intervention
Discussion
Gaps and Future Directions
Limitations
Conclusion
Declaration of Conflicting Interests
Funding
ORCID iD
References
Biographies
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In
Keywords
Rights and permissions
Authors
Metrics and citations
Metrics
Publication usage*
Total views and downloads: 2853
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 13 view articles Opens in new tab
Crossref: 14
- Health professionals’ knowledge and attitudes towards baby led weaning: A cross-sectional, exploratory, and observational study
- Timing of Complementary Food Introduction in the US National Survey of Children’s Health: Differences by Mother’s Nativity
- Early introduction of complementary foods among infants exposed to maternal incarceration in utero
- Reduction in the Introduction of Complementary Foods Prior to 4 Months and Prior to 6 Months: An Examination of the U.S. National Survey of Children’s Health 2016–2023
- Developmental Readiness for Complementary Feeding: Associations with Initiation Before Age 6 Months
- Masticación de alimentos duros y precisión articulatoria en niños de 6 a 8 años: resultados preliminares
- From store to home: Insights into parental baby snack choices
- Adherence to Introduction of Iron-Rich Solid Foods Recommendations for Infants: An Analysis of Canadian Community Health Survey Data Using Cycles 2015–2018
- Factors influencing parental decisions on food choices during complementary feeding: a qualitative study in Uruguay
- Infant Feeding Challenges in the First Six Months: Influencing Factors, Consequences, and Strategies for Maternal Support
- View More
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.
