As chronic conditions become incorporated into the family system, illness-oriented family processes that concern the dimension of time and belief systems influence coping.
Interweaving of Individual, Family, and Illness Development
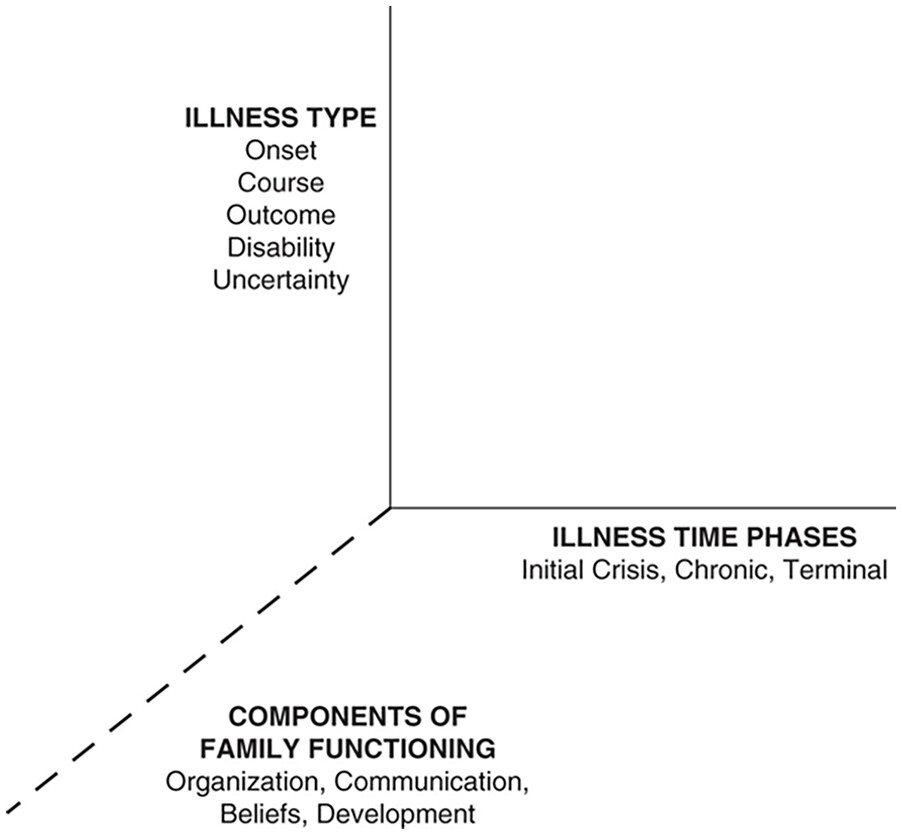
A developmental lens provides a powerful way to construct a normative framework for serious illness. To place the unfolding of chronic disease into a developmental context, it is vital to understand the intertwining of three evolutionary threads: illness, individual, and family development.
Concepts of human and family development have evolved from models that centered on a basic, somewhat invariant, sequence and unfolding of phases to ones that are more varied, fluid, and multidimensional, consistent with contemporary individual and family life course trajectories (
Lerner, 2018;
McGoldrick et al., 2016;
Walsh, 2012). Serious health conditions are one example of major, often unexpected, life challenges that can significantly alter the sequence and character of a family’s and its members’ life course.
Life structure, referring to the core elements in one’s life (e.g., work, childrearing, caregiving), is a useful central concept for both family and individual development. Illness, individual, and family development have in common the notion of phases, each with its own priorities and marked by the alternation of life structure stable and transitional phases (
Levinson, 1986). In a transition phase, one weighs different possibilities for personal and family life, eventually drawing up blueprints for the next phase, and then living them out. The actual possibilities may be affected by assets or barriers related to culture, race, class, gender, and sexual orientation. Transition phases can be quite fluid. Previous individual, family, and illness life structures are reappraised in the light of new developmental challenges. Furthermore, typical family development moves between phases that require intense bonding and an inside-the-family focus, as in early childrearing, and phases during which the external family boundary is loosened, such as with emerging young adults, often emphasizing increased personal identity and autonomy.
These unifying concepts provide a foundation for understanding the experience of chronic disorders. Life course development alternates between transition and life structure stable phases. And particular phases require relatively greater or lesser degrees of family cohesion. Illness, individual, and family development each pose priorities and challenges that move through phases of being more or less in sync with each other.
Serious health conditions tend to push developmental processes toward transition and increased need for cohesion and teamwork. Analogous to the addition of a new family member, illness onset sets in motion an inside-the-family-focused process of socialization to illness. Symptoms, loss of function, the demands of shifting or acquiring new illness-related roles, and the fears of further disability and/or death all push a family to pull together.
The need for family cohesion varies enormously with different illness types and phases. The tendency for a disease to pull a family inward increases with the level of disability or risk of progression and death. Progressive diseases over time inherently require greater cohesion than, for instance, constant-course illnesses. The ongoing addition of new demands with illness progression keeps a family’s energy focused inward, often impeding members’ development.
In clinical assessment, a basic question is: What is the fit between the psychosocial demands of a condition and family and individual life structures and developmental tasks at a particular point in the life course? Also, how will this fit change as the course of the illness unfolds in relation to the family’s and each member’s development?
Any transition in individual or family life course development will tend to magnify issues related to existing and anticipated loss. Transition periods are often characterized by upheaval, rethinking of prior commitments, and openness to change. Such times often hold a greater risk for the illness to become either embedded or ignored in planning for the next life phase. During a transition period, the process of thinking through future commitments can bring to the forefront family norms regarding loyalty through sacrifice and caregiving. The following example highlights this point.
In one second-generation Latino family, the father, a factory worker and primary financial provider, had a heart attack. His rehabilitation was uneventful, included appropriate lifestyle modifications, and a return to work. The family, including the oldest son, age 15 years, seemed relatively unaffected. Two years later, his father experienced a second more life-threatening heart attack and became totally disabled. His son, now 17 years old, had dreams of going away to college. The specter of financial hardship and the perceived need for a “man in the family” created a serious dilemma for the son and the family, which surfaced with precipitously declining academic performance and alcohol abuse. There was a fundamental clash between the developmental issues of launching a child and the ongoing demands of a progressive, life-threatening type of heart disease on the family. Furthermore, there is a resurgence of fears of loss fueled not only by the recurrence but also its timing with a major developmental transition for the oldest son. The son may fear that if he were to move away, he might never see his father alive again. There was a clash between simultaneous transition periods: (a) the illness transition to a more disabling, progressive, and life-threatening course; (b) the adolescent son’s transition to emerging adulthood with individuation, leaving home, and educational pursuits; and (c) the family developmental transition from the “living with teenagers” to a “launching young adults” phase. It also illustrates the significance of the type of illness: one that was less incapacitating and life-threatening might have interfered less with individual and family developmental priorities. At the time of initial diagnosis, inquiry about anticipated major transitions over the next 3 to 5 years and discussing them in relation to the specific kind of heart disease and its related uncertainties would help avert a future crisis.
It is essential to situate these developmental issues in the context of cultural values, socioeconomic considerations, availability of family or community resources, and access to health care. In many cultures, as in this Latino family, a strong emphasis on loyalty to family needs would normatively take priority over individual goals, especially with a major illness or disability.
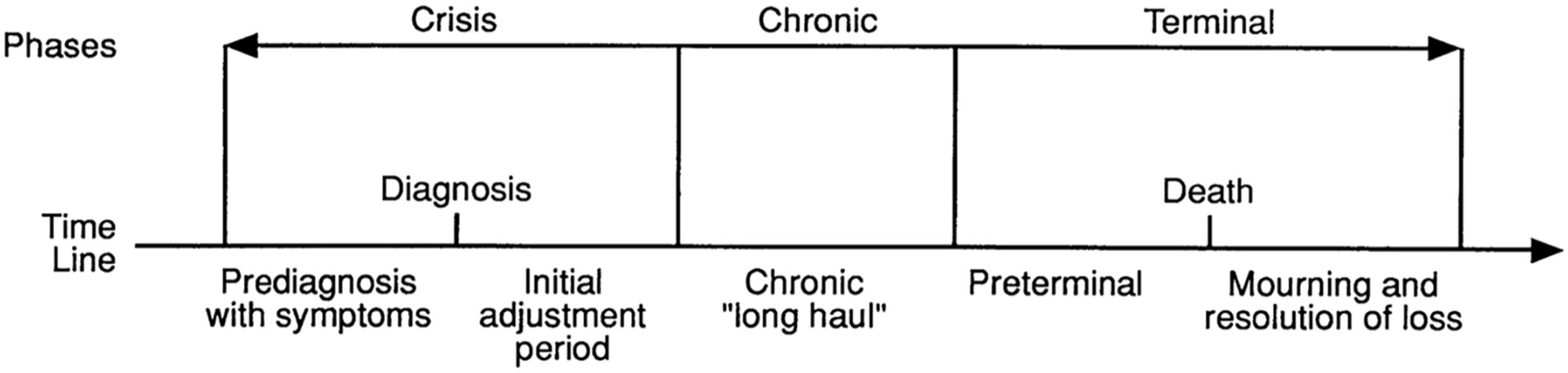
If the particular illness is progressive, relapsing, increasingly incapacitating, and/or life-threatening, then the unfolding phases of the disease will be punctuated by numerous transitions. In these situations, a family will need to alter its life structure more frequently to accommodate shifting and increasing demands of the disease. This level of demand and uncertainty keeps the illness in the forefront of a family’s consciousness, constantly impinging on its attempts to get back “in phase” developmentally.
The transition from the crisis to the chronic phase is the key juncture at which the intensity of families’ socialization to living with chronic conditions is often lessened. In this sense, it offers a window of opportunity for the family to reestablish or sometimes chart a “new normal” developmental course.
An overarching goal is to deal with the developmental demands of the illness while preserving family members’ own and the family’s development as a system over time. It is important to consider whose life plans were or might be canceled, postponed, or altered, and when plans put on hold and future developmental issues will be addressed. Using this framework, clinicians can anticipate developmental nodal points and offer prevention-oriented consultations. Family members can be helped to strike a healthier balance, with life plans that minimize feelings of guilt, over-responsibility, and hopelessness, and find family and external resources to enhance freedom both to pursue personal goals and to provide needed care for the ill member.
Health Beliefs
When illness strikes, families strive to create meaning for the illness experience that promotes competency and mastery (
Kleinman, 2020;
Rolland, 2018;
Wright & Bell, 2009,
2021). Since serious illness is often experienced as a betrayal of our fundamental trust in our bodies and belief in our invulnerability, it can be a formidable challenge to make meaning with an empowering narrative. Health beliefs can help us grapple with the existential dilemmas of our fear of death and tendency to deny our own mortality. They offer an approach to new and ambiguous situations, such as serious illness, and serve as cognitive maps guiding decisions and actions (
Hansson & Cederblad, 2004). Our appreciative inquiry into beliefs is a powerful foundation for collaboration with patients and families (
Rolland, 1997;
Wright & Bell, 2009,
2021). Growing research evidence shows that family members’ distress about illness and genetic risk is more closely associated with perceived risk or appraisals of seriousness than objective characteristics of the disease (
Franks & Roesch, 2006).
As part of early consultation(s), particularly in the initial crisis phase, it is useful to inquire about key family beliefs that shape families’ meaning-making, purpose, and coping strategies. This includes family health beliefs about: (a) normative illness experience; (b) meanings attached to symptoms by a family, ethnic group, religion, or the wider culture (e.g., chronic pain) or specific diseases (e.g., HIV/AIDS); (c) mind–body relationship, mastery, control, and acceptance; (d) assumptions about what caused an illness and what can influence it’s course and outcome; (e) multigenerational factors that have shaped a family’s health beliefs and response to illness; (f) gender-related beliefs about expected roles and behavior; and (g) anticipated nodal points in illness, individual, and family development when health beliefs will likely be strained or may need to shift. Clinicians should also consider the fit of health beliefs among family members as well as between the family and health care provider system and wider culture (
Kirmayer et al., 2015).
Normative Illness Experience
Illness beliefs about what is normative or dysfunctional can powerfully influence family adaptation. Family values that normalize psychosocial illness challenges without stigma facilitate their use of outside resources and maintain a positive identity. Help-seeking viewed as weak and shameful undercuts resilience and fosters suffering. Basically, with chronic conditions, difficulties are to be expected; mental health care and outside resources are often needed.
Two beneficial questions to elicit these beliefs are: (a) “How do you think other families would typically deal with a similar situation to yours?” and (b) “How do you think families ideally cope with your situation?” Families with strong beliefs in high achievement and perfectionism are prone to applying norms that are incredibly difficult to achieve with chronic conditions. Especially with untimely conditions that occur in childhood through early adulthood, there are additional pressures to keep up with socially expectable developmental milestones of age peers. The fact that developmental goals may take longer or need revision requires a flexible belief about what is normal and healthy. This kind of flexibility helps sustain hope.
Ethno-Cultural and Spiritual Beliefs
Ethno-cultural, racial, and spiritual beliefs and dominant societal norms can strongly influence family values, concerns about health and illness, and their pathways in healing (
Falicov, 2015;
Kirmayer et al., 2015;
Koenig, 2012;
Rolland, 2006a;
Walsh, 2010;
Wright, 2017). Significant ethno-cultural differences regarding health beliefs often emerge during a major health crisis. Since American families frequently represent a blend of different ethnic, racial, and spiritual beliefs, health care providers need to be mindful of the diverse belief systems of various subpopulations in their communities, particularly as they are often expressed in different behavioral patterns. For instance, cultural and religious values and expectations can vary as to: (a) the appropriate “sick role” for the patient; (b) the kind and degree of open communication about the condition and prognosis; (c) who should be included in the illness caregiving system (e.g., extended family, friends, professionals); (d) gender-based expectations for caregiving and the primary caregiver (most often wife /mother/daughter/daughter-in-law); (e) which treatment or healing approaches can be helpful [e.g., Western medical experts, faith healing practitioners, mindfulness meditation (
Kabat-Zinn, 2023), Eastern or indigenous traditional beliefs about illness etiology and curative practices]; (f) proper rituals at different illness phases (e.g., hospital bedside vigils, healing, and funeral rituals); and (g) within-family diversity (e.g., parents’ Spanish and Mexican cultural differences in handling a son’s diabetes). It is especially important to be mindful of beliefs with racial minority groups (e.g., African American, Asian, Hispanic) that experience discrimination or marginalization from prevailing Euro-American culture.
Clinicians need to be mindful of cultural and religious differences between themselves, the patient, and the family to forge a workable alliance through a long-term condition. Effective collaboration occurs when providers inquire into families’ cultural and spiritual beliefs about illness and healing. Disregarding these issues can lead families to distance themselves from health care providers and available community resources—a major source of adherence issues and treatment failure. Sometimes, providers need to flexibly modify their professional ethos to be “in charge.” This entails tolerance that patients, not health care providers, retain final decision-making about their bodies.
Beliefs About Mastery and Control Facing Illness
It is beneficial to inquire how a family defines mastery or control in general and particularly with illness. A family may hold different beliefs about control when dealing with some diseases in contrast to other life challenges. By example, regardless of the actual severity or prognosis in a particular case, cancer may be equated with “death” or “no control” because of medical statistics, cultural myth, or family history. In contrast, families may have enabling stories about a relative or friend, who despite cancer and a shortened lifespan, lived a “full” life centered on effectively prioritizing the quality of relationships and goals. Clinicians can highlight such positive narratives to help counteract cultural beliefs that may equate success with control over a disease.
A family’s beliefs about control can affect treatment adherence and the family’s participation in a member’s treatment and healing process. When patients view disease course or outcome as a matter of chance or beyond their control, they tend to establish marginal collaboration with health care providers and may not adhere to treatment recommendations. When poor minority families receive inadequate or lack access to care, it often fosters a fatalistic attitude and minimal engagement with providers, who may not be trusted. Because any therapeutic relationship depends on shared beliefs about what is therapeutic, it is essential to establish a workable accommodation of core beliefs among the patient, family, and health care team. Families that feel misunderstood by health care providers are often reacting to a lack of collaboration at this basic value level.
The quality of fit between family beliefs about mastery and the relative need for provider and technological care can vary with the illness phase. For some conditions, the crisis phase involves protracted care outside the family’s direct control. This may be stressful for a family that prefers to tackle its own problems without outside involvement and control. The patient’s return home, often part of the transition to the chronic phase, allows members to reassert their competence and leadership more fully. By contrast, a family that is more comfortable with intense involvement by health care providers might experience more difficulty when their ill member returns home from a rehabilitation facility, losing their locus of competency, the professional caregiving system. Appreciation of such normative differences in beliefs about control helps guide an effective psychosocial treatment plan tailored to family preferences.
Family Beliefs About Illness and Disability Etiology
When a major health issue arises, most of us question, “Why me (or us)?” and “Why now?” (
Roesch & Weiner, 2001). We try to develop an explanation or story that helps organize our experience. With the limits of current medical knowledge and immense uncertainties about the relative importance of myriad factors, individual members and families construct diverse causal attributions about a condition. Beliefs about etiology need consideration separately from beliefs about what can affect the outcome. It is vital to inquire about
each family member’s perspective. Various explanations may include the biological (e.g., virus), religious, societal (e.g., poverty or pollution), or individual or family dysfunction. Beliefs about etiology can include punishment for earlier misdeeds (e.g., an affair, an ancestor’s transgressions), blame of a particular family member (“Your nagging gave me a heart attack!”), a sense of injustice (“Why am I being punished”), genetics (e.g., heart disease runs on one side of the family), negligence by the patient (e.g., smoking) or by parents (e.g., sudden infant death syndrome), religious beliefs (God’s punishment for sinful living), or simply bad luck. Inquiry about culturally based beliefs or syndromes is valuable. For instance, Latino families may believe that nervios, an increased susceptibility to stress and symptoms of nervousness, has caused a cancer.
Optimally, family narratives respect the limits of scientific knowledge, affirm basic competency, and promote the flexible use of multiple biological, psychosocial-spiritual healing strategies. In contrast, causal attributions that invoke blame, shame, or guilt are particularly important to uncover, as they can derail family coping and adaptation. With a life-threatening illness, a blamed family member may be held accountable if the patient dies (e.g., “You neglected his care!”). Decisions about treatment can become confounded and filled with tension. The following case vignette illustrates how self-blame may remain hidden and the importance of early inquiry by health care providers:
Anne and Jack, a young couple, have one child Ellen, aged 5, who is terminally ill with leukemia. The pediatric oncologist has offered the parents the choice between an experimental treatment with a low probability of success, or halting treatment. Jack’s position is “Let’s stop; enough is enough.” Anne, on the other hand, felt, “We must continue; we can’t let her die.” The couple cannot reach an agreement, and the physician is immobilized. She requests a consultation for the couple.
When asked, “How do you each try to explain or make sense of how your daughter got leukemia?” critical stories emerge. Jack basically sees it as bad luck. Anne, however, has a very different belief. During her pregnancy with Ellen, Anne’s father had a heart attack and died several months later from a second episode. Anne experienced this as a time of great stress and grief, which she felt adversely affected Ellen’s intrauterine life. After Ellen’s birth, by normal delivery, Anne was still mourning the loss of her father and feels that this negatively affected the quality of her bonding with Ellen and led to a hidden depression in her infant. Further, Anne had read research linking depression with decreased immune system effectiveness, which could then decrease normal surveillance and clearing of cancer cells from the body. She believes this combination of factors caused her child’s cancer and that if she had been a more competent mother, this never would have happened. Anne said she had never told this story to anyone, including her husband, because no one had ever asked, and she was very ashamed. She had hoped for a cure, so that the whole issue could be resolved. She could not accept stopping treatment because, to her, it meant that Ellen’s death would then be her fault. This wrenching situation could have been averted had someone on the healthcare team inquired early on regarding any beliefs about the etiology of Ellen’s cancer. Early timely referral to a family therapist would have been optimal.
Belief System Flexibility
Because illnesses vary enormously in their physiological responsiveness to psychosocial factors,
both families and providers need to distinguish beliefs about (a) overall participation (or active agency) in a long-term disease process and (b) ability to control the biological progression and outcome. Families’ experience of competence often depends on their grasp of these distinctions. Mindful of advances in positive psychology (
Carr et al., 2024), optimal family, and provider narratives respect the limits of scientific knowledge, affirm basic competency, and promote the flexible use of multiple biological and psychosocial healing strategies.
Clinicians can encourage a family’s flexible involvement in the overall illness and treatment process independent of whether a disease is stable, improving, or in a terminal phase. Proactive efforts to influence the course can make a difference, such as when parents stop serving sweet desserts, so as not to tempt an adolescent with diabetes. If an ill member gets a cancer recurrence and enters a terminal phase, involvement as an expression of mastery transitions from influencing the outcome to easing suffering and supporting palliative care.
Flexibility within the family and the health care team is a key variable in optimal functioning. Rather than linking mastery in a rigid way with biological outcome (survival or recovery), families can define mastery in a more “holistic” sense. Involvement in the overall process can be the main criteria of success. Psychosocial-spiritual healing may influence the course and outcome, but a positive disease outcome is not necessary for a family to feel successful. This flexible view of mastery permits the quality of relations within the family, or between the family and health care team, to become a central criterion of success. Health care providers’ competence is valued from both a technical and caregiving perspective, not solely from the biological disease course.
Families with the strongest and most rigid beliefs about control and personal responsibility may adapt well during earlier illness phases but become vulnerable if the condition progresses and beyond their control. A mind-set of “We understand the risks, and we are going to try our best to beat this cancer” promotes resilience, while “We must beat cancer or we’ve failed” fuels a feeling of defeat.
Fit Among Health Care Provider, Health Care System, and Family Beliefs
The same questions asked of families concerning beliefs are relevant to each of us on the health care team:
1.
What key values and health beliefs guide you in life? Clinicians also need to consider their own experiences and feelings about illness and loss (
McDaniel et al., 1997;
Rolland, 2018). Awareness and ease with our own multigenerational family history with illness and loss, our health beliefs, and our current developmental phase will enhance our ability to work effectively with families facing serious illness.
2.
What professional discipline and health care setting values guide you as a clinician?
3.
What are your views about both yours and the family’s ability to influence the illness course and outcome?
4.
How do you envision the balance between your and the family’s involvement in the treatment process? How can core belief differences be bridged?
Commonly, belief differences among family members or with the health care team emerge at major treatment or illness transition points. By example, in situations of severe disability or terminal illness, one family member may want the patient to return home, whereas another prefers transfer to an extended care facility. Because the primary caregiver role is typically assigned to the wife/mother, she is the one apt to bear most burdens in this regard. Anticipating the collision of gender-based beliefs about caregiving with the potentially overwhelming demands of home-based care for a severely disabled family member can help families flexibly modify their rules and avert the risk of family caretaker overload, resentment, and deteriorating family relationships.
The murky boundary between the chronic and terminal phase highlights the potential for providers’ beliefs to collide with those of the patient and family. Families may not know how to interpret continued life-saving efforts, assuming real hope where virtually none exists. Clinicians can feel governed by a technological obligation that requires them to exhaust all available treatments, regardless of the odds of success. The health care team can have its own difficulties stopping treatment. Continued treatment inertia can represent the health care team’s difficulty separating a core belief in controlling diseases from their beliefs about involvement (distinct from cure) in a patient’s total care, which includes bio-psycho-social-spiritual wellbeing.