

Nurse-Led Medication Management for Older People in Home Care: A Systematic Review of Evolving Nurse Responsibilities in Technology-assisted Care
Abstract
Introduction
Methods
Design
Protocol and Registration
Literature Search
Selecting Relevant Studies
Quality Appraisal
Research Synthesis
Ethical Considerations
Results
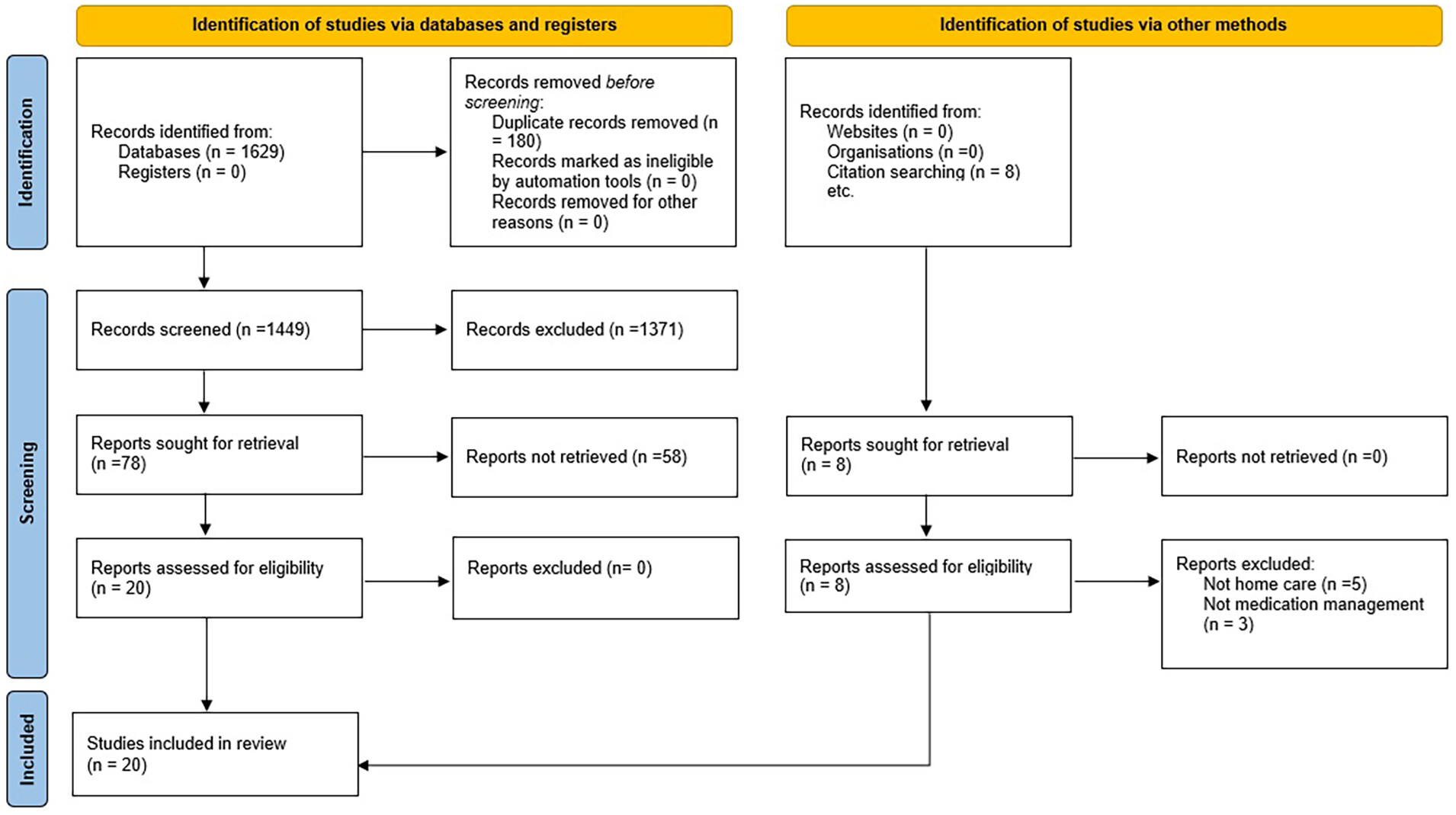
Search Outcome and Study Selection
Methodological Quality Appraisal
General Characteristics of Included Studies
| Author/country | Research methodology | Sample/setting | Type of technology-assisted care | Nurse qualification | Nurse’s role in medication management |
|---|---|---|---|---|---|
| Blum and Gottlieb34/USA | Randomized trial | 204 Elderlies/own home | Telemonitoring Philips Electronics E-care System for remote monitoring, telephone | Heart failure nurse practitioner | Medication review |
| Delaney et al46/USA | Pilot study/quasi-experimental | 50 Patients in the intervention (n = 26) and control group (n = 24), 49 years to above 90 years with most patients (71%) between the ages of 70 and 90/own home | Physiological telemonitoring system | Nurse trained in heart failure | Medication review |
| Marek et al42/USA | Randomized, controlled, three-arm longitudinal study | Older adults from elderly care home health care (n = 414)/own home | Medication-dispensing machine | APNs and RNs coordinated care for drug screening to identify interactions | Medication dispensing |
| Feldman et al38/USA | Three-arm cluster randomized trial | 845 Patients as elderlies/own home | Home care field nurse | Medication assessment, monitoring, education and self-management support | |
| Grubbs et al40/USA | Randomized control trial | Veterans (n = 132) with posttraumatic stress disorder recruited from 5 large- (5000-10,000 patients) and 6 medium-sized/own home, community-based outpatient clinics | Telemedicine: inter-active video | Psychiatric advanced practice nurse | Medication review |
| Ögren et al44/Sweden | Randomized controlled trial | 660 Older people in the intervention and control group/own home | Telephone follow up | Practical nurse | Medication titration |
| Persell et al43/USA | 3-Group cluster randomized clinical trial | 794 Participants/own home | EHR, telephone | Nurse educator | Medication therapy management |
| Cheville et al36/USA | 3-Arm randomized clinical trial | 516 Elderlies/own home | Telerehabilitation, telephone or fax communication | Nurse pain care manager | Pharmacological pain management |
| Gordon et al47/Canada | A pragmatic, multimethod feasibility study | 26 Participants/own home | Smartphone-based telemonitoring app | Clinical nurse | Medication review |
| Kazawa et al41/Japan | Post-hoc analysis of randomized controlled trial | 40 Company employees: intervention group (n = 21), control group (n = 19)/own home | Telenursing, video | Corresponding nurse | Medication review |
| Bouleftour et al35/France | A randomized, multicentre, controlled trial | 183 Patients elderlies: 92 and 91 patients to intervention and control groups/own home | Telephone follow-up | Trained nurse | Adherence to medication, management of potential drug toxicities |
| Stacey et al49/Canada | Quality improvement | 113 Audio-recorded calls for patients aged 64 years/own home | Telephone | Oncology nurse | Medication review, relevant to symptoms |
| Coskun and Duygulu37/Turkey | Randomized control trial | 66 Elderly patients in the intervention (n = 33) and control (n = 33) groups/own home | Telephone follow up at sixth month of discharge | Clinical nurse and coordinator nurse | Medication review |
| Ghobadi et al39/Iran | Clinical trial | 94 HF patients with comorbidities: intervention (n = 47) and control (n = 47)/own home | Telephone follow-ups | Experienced nurse in heart failure | Medication instructions |
| Huang et al48/China | Quasi-experimental, non-equivalent, two-group, comparison group design | 339 Patients in the intervention and 333 patients in the control group/own home | Cloud clinic, app and telephone follow up for online insulin injection activities | Clinical nurse | Insulin therapy |
| Jun-O'Connell et al45/USA | Cohort | 447 Consecutive stroke patients/own home | Telephone | Stroke nurse navigator | Medication review |
| Kajander-Unkuri et al33/Finland | A pragmatic non-randomized controlled clinical trial | Intervention groups and control groups (n = 64 and 46 elderly people)/own home | Robot for medication management | Public health nurses, practical nurses, and registered nurses | Loading medications inside the robot enabling older home care clients to carry out medication management |
| Sison et al50/USA | Quality improvement initiative | 35 Veterans as elderlies/own home | Telephone-based intervention | RN with geriatric experience in inpatient, outpatient, and home care settings, discharge coordinator and transitional care case manager | Medication reconciliation |
| Turjamaa et al52/Finland | Qualitative interview study | 38 Older home care clients/own home | Robot for medication management | Practical nurse | Dispensing medications |
| Turjamaa et al51/Finland | Qualitative focus group interview study | 62 Home care professionals/own home | Robot for medication management | Practical nurse | Dispensing medications |
Nurse-Led Initiatives for Medication Management in Technology-assisted Home Care
| Author | Outcome of the intervention for medication management | Nurse’s role within the multidisciplinary team | Patient safety indicator | Implications for patient safety |
|---|---|---|---|---|
| Blum and Gottlieb34 | No difference in 30-day readmissions (P = .627) or mortality (P = .575) between the groups, improvement of quality of life over time but without differences between the groups (P > .05), no differences in Medicare payments for inpatient or emergency department visits, and length of stay, percentage of patients readmitted within 30 days was initially lower with telemonitoring during the first year, but this effect did not persist over time | Nurse practitioner and consultation with a cardiologist | Quality of life, readmission, costs | Maintaining communication, offering encouragement, and addressing any inquiries with the probable impact on unnecessary readmissions and referral to the hospital |
| Delaney et al46 | Improved understanding of medication (M/SD: 3.83, 0.491, P < .001); non-significant trend toward improved quality of life and fewer hospital readmissions (9 vs 6 patients) | Nurse-directed multicomponent home care intervention and cardiac program manager and referral to the physician | Medications—prescription and over the counter drugs, readmission | Education, assessment, remote-monitoring, and therapeutic activities based on the self-care model to develop own daily routine and regularly take medications |
| Marek et al42 | Pill organizer intervention cost $151 monthly, resulting in savings of $296 monthly or $3552 annually. Medication-dispensing machine intervention cost $251 monthly, with Medicare costs $409 higher monthly compared to the pill organizer group | Care coordination by advanced practice nurses and RNs involving physicians, pharmacists, social workers, and other service providers; medication screening by pharmacist and advanced practice nurses | Pill organizers helped in organizing and remembering medication schedules, while medication dispensing machines were preloaded with medications in reusable plastic cups | Evaluations and care plan encouraging patients and their families for medication self-management behaviors, frequent communication between the medication management team and the patient |
| Feldman et al38 | No significant differences at the 12-month mark in BP control rates (control: 25% vs intervention: 22%), systolic BP (143.8 mmHg vs 143.9 mmHg), and medication intensification rates (47% vs 54%); compliance score ranged from 11.5 to 11.7 indicating a significantly higher level of medication adherence | Home care nurse, and health educator along with the primary care physician | Medication intensification as taking new medications, and patient-reported hypertension self-management | Hypertension medication assessment, monitoring, education, and self-management support, the nurse collaborated with home care nurses to enhance patients’ comprehension of their hypertension risk factors and medication routines, encouraging them to convey their concerns to their personal physicians |
| Grubbs et al40 | Collaborative care: 72% at least one medication management session in year, 30% via interactive video, 3.7 encounters per year | Two to third of medication management encounters with the nurse and the rest with the prescriber | Medication management encounters | Providing high rates of medication management encounters, including remote sessions via interactive video without onsite mental health services |
| Ögren et al.44 | A higher percentage of the intervention group compared with the control achieved the treatment goal for BP (systolic: 79.4% vs 55.3%, P < .001; diastolic: 90.3% vs 77.9%, P < .001) and for LDL-C (69.3% vs 48.9%, P < .001) | Practical nurse along with a consultant physician | Compliance with the treatment and reaching the target LDL-C and BP based on individual-adjusted medications | Improved medication titration and the proportion of patients that reached the treatment target at follow up, creating the opportunity to discuss their treatment and potential side effects with the nurse, likely increasing medication adherence. The intervention’s positive outcomes are attributed to reduced therapeutic inertia and improved adherence |
| Persell et al43 | In the electronic health record plus education group, systolic BP was lower compared to the EHR-alone group (−5.6 mmHg; 95% CI: −8.8– to −2.4 mm Hg), at 12 months, greater medication reconciliation for hypertension medications (OR: 2.0 [95% CI: 1.3-3.3; P = .003]) and all long-term medications (OR for both comparisons, 2.5; 95% CI: 1.2-5.2; P = .02) were in the electronic health record plus education group, understanding of medication instructions and dosing was higher in the electronic health record plus education group compared to the usual care group for hypertension medications (OR: 2.3; 95% CI: 1.1-4.8) and all medications combined (OR: 1.7; 95% CI: 1.0-2.8), reconciliation of all medications was higher in the electronic health record plus education group compared to the usual care group (OR: 6.0; 95% CI: 1.1-32.2; P = .04). | Nurse educator and communicating the review results to the clinician and planning for referral | Identifying possible medication errors such as duplicates or internal discrepancies, and pinpoint areas requiring monitoring and subsequent follow-up, medication comprehension assessments, medication usage patterns, reconciling with electronic health records, consolidating dosing regimens, and creating medication tables for complex regimens, assessing adherence, improper usage patterns, and reasons for nonadherence | Improving patients’ understanding of their chronic conditions, addressing misconceptions and the importance of medications, medication education and review, proactive follow up by the nurse, combining EHR with nurse-led self-management education causes greater reductions in BP demonstrating the importance of understanding of medication instructions and dosing |
| Cheville et al36 | Reduction in pain interference (−0.4; 95% CI: −0.79– to −0.10; P = .01) and average intensity (−0.5; 95% CI, −0.84– to −0.11; P = .006), higher odds of home discharge (OR, 3.8; 95% CI, 1.1-12.4; P = .03) | Nurse-coordinated pharmacological pain management by a nurse pain care manager in collaboration with a physical therapist-physician team as general internist and a palliative care physician/medical oncologist | Tracking pain and treatment recommendations | Improving function and better pain control via collaborative telerehabilitation within a multidisciplinary team |
| Gordon et al47 | 56%, 55%, 72% of heart failure, hypertension, and diabetes mellitus, maintained adherence to physiological readings, respectively | Nurse-led care and connecting the patient to the clinical team to address symptoms, cross-condition needs, and concerns | Adherence to self-monitoring and medication use | Improving patient-clinician communication and connecting to the personal clinician, visualizing live data, and assuring patients that the team was taking care of their health, receiving immediate feedback, proactive calling by the nurse |
| Kazawa et al 202041 | Comparing medication intake and improvement in main clinical indicators, the distance method was equally effective as the direct face-to-face method (95% CI: −3.50 (−8.92 to 1.92)) | Education by the corresponding nurse for self-monitoring medications and management | Self-management behaviors | Self-management as to take or inject medications daily and taking the necessary action in case of missing the dose self-management behaviors |
| Bouleftour et al35 | Medium medication adherence (81.3%), reduction in the number of patients experiencing grade 3 adverse events during the follow-up period (18.5% vs 33%; OR: 0.45 [95% CI: 0.23, 0.9]; P = .03). Toxicities were mild to moderate (grade 1 and grade 2), with asthenia and pain being the most common. Improvement in mucositis, rash, and anorexia with no effect on diarrhea and nausea symptoms | Monitoring and follow up by the nurse and further referral to the physician | Identifying toxicities and expected adverse effects | Early identification and improvement in grade 3 toxicities’ management to enhance adherence to medications |
| Stacey et al49 | Symptoms resolved (38%), worsened (25%), remained unchanged (3%), or had unknown status (33%). Eight patients (13%) visited the emergency department | Documentation of cancer-related symptoms receiving therapies and medications by the nurse using a chart audit for referral to the oncologist | Review of medications relevant to the symptom, patient agreement/commitment to continue or initiate medications | More possibility to work within nursing scope of practice and less inclusion for the immediate referral of patient-reported symptoms to oncologists, lack familiarity or comfort with nurse role’s scope without the remote support tool |
| Coskun and Duygulu37 | Higher level of functional autonomy and quality of life of patients at ninth week (P < .05), less repeated hospitalization (n = 2) or emergency service referral (n = 1) at the 6-month follow-up (P < .05) for medication adjustments | Nurse led transitional care model team: physician, clinic nurses, coordinator nurse, physiotherapist, dietician, caregiver/family member | Functional autonomy, quality of life levels, and repeated admission/re-hospitalization rates to the clinic | Coordinated care planning by the multidisciplinary team and consultancy at post-discharge care |
| Ghobadi et al39 | Mean changes in total scores of symptom burden and medication adherence at various time points (P < .001) indicating an increase in medication adherence and reduction symptoms’ burden | Multidisciplinary management program supervised by the nurse consisting of cardiologist, clinical pharmacist, and nutritionist | Self-management and self-monitoring and multi-drug management | Liaison role between patients and the multi-professional management team, managing new and multiple symptoms in comorbidities, and directing the patient to overcome obstacles to adherence to numerous medications |
| Huang et al48 | At 3 and 6 months after the intervention, significant differences in compliance rates for fasting BP (sixth month rate difference: 0.077, 95% CI: 0.007-0.14, P < .05) and HbA1c (%) (sixth month rate difference: 0.106, 95% CI: 0.324-0.180, P < .01) between the intervention and control groups, “my opinion on Insulin” scale was in the group was (intervention: 80.18 ± 6.68 vs control: 71.15 ± 8.17; mean difference: 9.03, 95% CI: 7.900-10.160, P < .01), daily insulin dosages sixth month: Intervention M/SD: 16.10 ± 3.12 and control: 18.25 ± 3.32 (mean difference: 2.14, P < .01) | Nurse-led video education regarding insulin injection activities | Reduction of the patient’s daily insulin dose and improvement of the patients’ compliance using insulin therapy | Implementing a safe, standardized, and consistent approach to patients with diabetes mellitus undergoing initial basal insulin therapy during post-discharge follow-up |
| Jun-O'Connell et al45 | A greater utilization of mechanical thrombectomy (35.6% vs 24.7%, P = .016), lower usage of pre-admission oral anticoagulants (1.3% vs 5.6%, P = .025), and a lower frequency of previous stroke/transient ischemic attack (14.4% vs 27.5%, P = .001), lower 30-day unplanned readmission rates (log-rank P = .029), with reduced risks of such readmissions (adjusted HR 0.48, 95% CI 0.23-0.99, P = .046) | Medication review and discharge plan verification follow up by the nurse along with support and confirmation by the neurologist and discharge physicians | Medication usage and side effects and complications, readmission | Standardized follow-up transition plan, verification of medications for post-discharge use, and an early identification of complications |
| Kajander-Unkuri et al33 | Number of home visits significantly reduced by 89.4% at the 1-month follow-up (from 878 to 93 visits) and by 92.5% at the 2-month follow-up (from 878 to 66 visits, P < .001) | Dispensing medications for home care use by the pharmacist, and manual dispersion of medications to the dosette by the nurse | Dispensing right medications at right times, monitoring medication use at home | Reduced time spent on medication management leads to less time available for tasks such as ordering medications, monitoring their effects, and providing medication education |
| Sison et al50 | Nine medication discrepancies in 8 patients (22.9%), with an average of 1.1 discrepancies per patient; 5 discrepancies (56%) due to incomplete medication reconciliation at discharge, and 5 (56%) had potential for serious harm, a higher percentage of patients received a post-discharge call within 7 days (82.9% vs 61.9%; P = .03). Of 35 veterans participating in the program, the nurse identified 9 medication discrepancies in 8 patients (22.9%; average of 1.1 discrepancies per patient) | Nurse as discharge coordinator and transitional care case manager to perform detailed medication reconciliation, follow-up with primary care physician, geriatricians, and pharmacist | Medication reconciliation | Serving as a central contact for the patient’s post-discharge care involving consistent communication with various stakeholders regarding the patient’s requirements, medication supply, and offering guidance and education to the patient and caregiver, identifying medication discrepancies, and appropriate intervention to prevent harm |
| Turjamaa et al52 | Positive experiences with medication technology but caused daily life challenges; implementation required practice with a nurse; participants felt excluded from the development process | Pharmacists dispensed medications for home care, while nurses manually prepared medication doses in dosette | Accurate dispensing of medications at the correct times and allowed for monitoring of medication usage at home, maintaining an electronic record of medication use | Ensuring a safe medication process, scheduling daily routines, fostering independence from home care professionals’ schedules, minimizing the impact on professionals’ busy work, no need for memorizing medications, but the challenge of medication use on a trip |
| Turjamaa et al51 | Home care professionals required competence including familiarity with digital solutions, addressing preconceived attitudes, and assessing the robot’s suitability for older individuals while advising on its usage | Pharmacists dispensed medications for home care, while nurses prepared doses in dosette | Experiences of the implementation, use and competence needs of a robot | Enabling home care professionals to schedule and conduct visits more flexibly, the robot was accessible 24/7, offering individual training opportunities, written and illustrated information sheets enhanced understanding of robot usage, need for improving proficiency and competence in the digital health, access to experts should be ensured during holidays to safeguard the medication process |
Fundamental principles
Nurses and their role identities
Enhanced care quality and medication safety
Discussion

Limitations
Conclusion
Acknowledgments
Ethical Approval and Informed Consent Statements
Declaration of Conflicting Interests
Funding
ORCID iDs
Data availability statement
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In

Keywords
Rights and permissions
Data availability statement
Article versions
Authors
Author Contributions
Metrics and citations
Metrics
Journals metrics
This article was published in Home Health Care Management & Practice.
View All Journal MetricsPublication usage*
Total views and downloads: 4788
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 4 view articles Opens in new tab
Crossref: 3
- Nurses' role in deprescribing for older adults: A scoping review
- Robot-assisted medication management in home care and long-term care settings: a mixed-method systematic review
- Therapeutic Inertia in Nursing: A Concept Analysis
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.
