As of July 2022, approximately 70% of Americans were unvaccinated, had not completed their primary series, or had not gotten a booster dose (
Rouw, 2022). Misinformation about COVID-19 and COVID-19 vaccines has spread on social media and resulted in increases in vaccine hesitancy (
Jennings et al., 2021;
Puri et al., 2020). There is a need to address the problem by developing and implementing interventions to promote vaccine uptake, especially on social media (
Limaye et al., 2021;
World Health Organization, n.d.).
Most prior interventions aimed at promoting vaccination have targeted patients (e.g., with patient appointment reminders by text message), providers (e.g., trainings and EHR modifications), and institutions (e.g., educational systems with laws requiring vaccination for school registration) (
Batteux et al., 2022;
Jacobson Vann et al., 2018). Among interventions aimed specifically at the vaccine hesitant, approaches have largely been provided face-to-face during home visits or at a clinic. Such interventions have been found to be effective in improving vaccination and, to a lesser extent, improving knowledge about vaccination (
Kaufman et al., 2018).
Attempts to combat vaccine hesitancy have not traditionally taken advantage of the affordances of social media platforms and especially, the opportunity for public health practitioners to interact directly with the vaccine hesitant on social media (
Limaye et al., 2021;
Petkovic et al., 2021) and none to our knowledge around the COVID-19 vaccine. Studies that have used social media to study vaccine promotion have found positive effects on vaccine knowledge, attitudes, and intentions/behaviors (
Limaye et al., 2021). However, most of these trials have used lab-based experiments to mimic social media environments. Studies are needed that investigate changing beliefs and attitudes and in real-world social media environments (
Abroms, 2019).
Furthermore, prior studies of vaccine promotion on social media are limited in their approach as they have largely sought to investigate the effects of correcting or debunking falsehoods or altering other aspects of the social media environment (
Abroms, 2019;
Liao et al., 2020;
Limaye et al., 2021). Although debunking is an important component of addressing vaccine misinformation, communications must also be developed that build trust and address deep-seated reasons for vaccine hesitancy (
Larson et al., 2018). One strategy to do this is through empathetic engagement, a communication approach that involves actively listening to and understanding the perspectives, emotions, and experiences of those with opposing views. According to
Larson et al. (2018), empathic engagement offers an effective way to build trust, which in turn can be the foundation of attitude change and health behavior change, especially in the case of deep-seated views against vaccination (
Larson & Broniatowski, 2021a,
2021b;
Larson et al. 2018).
In summary, few studies on social media have focused on vaccine promotion, approached it in a way that directly addresses individuals’ concerns (
Larson & Broniatowski, 2021a,
2021b;
Reyna et al., 2021), or been conducted in actual social media environments (
Limaye et al., 2021). To adequately address misinformation and build trust, it is important to demonstrate understanding of audiences’ concerns, tailor responses to their specific concerns, communicate the gist of these responses (
Reyna et al., 2021), and address them in spaces where people are already receiving other health information, such as on social media (
Abroms, 2019). There is a critical need for research to evaluate such interventions in popular social media settings, such as Facebook.
The current study evaluated the efficacy of a social media intervention to increase uptake of COVID-19 vaccines by providing information about COVID-19 in a manner that elicits concerns and builds trust. Specifically, we evaluated the efficacy of a moderated private Facebook discussion group about COVID-19 vaccines compared with referral to Facebook’s COVID-19 vaccine information center. Primary outcomes at 6 weeks consisted of COVID-19 vaccine uptake, intention to vaccinate for COVID-19, and intention to encourage others to vaccinate for COVID-19. Secondary outcomes included improvements in intention to vaccinate for COVID-19, general vaccine confidence, COVID-19 vaccine confidence, responsibility for vaccination to others, and engagement with posts.
Methods
Enrollment Procedures and Sample
In January–April 2022, participants were recruited using Amazon’s Mechanical Turk (MTurk). MTurk workers who lived in the United States were paid US$0.40 to take an eligibility survey and told that, if eligible, they could take longer surveys, earn gift cards, and join a Facebook group to learn about and discuss vaccines. Participants were eligible for recruitment if they were 18 years or older, had not received a single dose of the COVID-19 vaccine, and were daily Facebook users. In addition, to avoid fraudulent enrollees, participants needed to pass an attention check to see whether they were reading the question, identify the zip code for their reported state of residence, and provide a valid Facebook account and email address.
Eligible participants who verified their email and consented to participate in the study were asked to complete a baseline survey and then randomized. Eligible participants were emailed a link to request membership in their assigned group. Participants were considered enrolled in the study after group administrators accepted their Facebook membership request and they joined the group. Enrolled participants were sent follow-up surveys at 2, 4, and 6 weeks after their enrollment. Participants were reimbursed with Amazon gift cards for surveys (US$20 for the baseline survey, US$25 for the 2-week survey, and US$30 for the 4- and 6-week surveys with addition US$5 for answering the survey within 24 hours). Results presented in this analysis are for the baseline and 6-week surveys.
Participants were recruited and offered the intervention in two waves. Wave 1 was run from January 17, 2022 to February 18, 2022, and participants were randomized to intervention or control Facebook groups. In Wave 1, we targeted enrollment of 150 participants/group. Wave 1 randomization resulted in 6,645 people screened, 484 randomized, and 353 enrolled (
Figure 1). Wave 2 was run from February 15, 2022 to March 13, 2022. The enrollment target for Wave 2 was reduced from 150 because moderators felt smaller groups would be more manageable. In addition, for Wave 2, participants were randomized to an additional intervention group where participants could not initiate their own posts within the Facebook group. As the two intervention groups from Wave 2 were very similar in practice with no one initiating posting in either intervention group, the intervention groups were collapsed into one intervention condition for analysis. In Wave 2, we targeted enrollment of 50 participants per group. Wave 2 randomization resulted in 3,894 people screened, 235 randomized, and 155 enrolled across the three groups.
During the analysis phase, 30 participants were removed from the analysis. This was because 15 intervention participants and 14 control participants gave inconsistent answers on the primary outcome related to vaccine uptake at 4 weeks, which seemed fraudulent (e.g., they indicated that they were unvaccinated on the screener, but then reported receiving three vaccine doses at the 4-week follow-up). Because of these inconsistencies, a decision was made to remove these participants from the sample. One person enrolled in Wave 2 was removed from analysis because they participated in Wave 1. Waves 1 and 2 were pooled for analysis purposes. The final sample size across the two waves was N = 478.
Interventions
Participants in both groups received a link to a private Facebook group and referral to a Centers for Disease Control and Prevention (CDC) webpage on COVID-19 vaccination. All Facebook groups were titled similarly (e.g., “Conversations About Vaccines”), so that, participants could not tell if they were randomized to intervention or control. Once they joined, they were able to see the content in their assigned group.
Intervention
Participants in the intervention group were given two to three vaccination posts/day for 28 days (4 weeks) for a total of approximately 60 posts. Project staff served as group moderators and responded daily to comments and original posts made by group members. Because of Facebook’s design features, posts made in the group also presumably showed up in a participants’ Facebook Newsfeed, allowing participants to see the post and comment/like the post as they scrolled through their Newsfeed.
Posts were aimed at educating about COVID-19 risks and COVID-19 vaccination, soliciting concerns around COVID-19 vaccination, and engaging group members. Posts about the risks of COVID-19 and COVID-19 vaccination were crafted according to Fuzzy Trace Theory (
Reyna et al., 2021), a leading empirically validated theory of medical decision-making that emphasizes the importance of communicating about risks and doing it in a way that communicates about the gist, or bottom-line meaning, of risks more than communicating verbatim information about risks (e.g., primarily facts and statistics). This method of crafting messages was chosen because evidence exists that people are more likely to retain and use bottom-line information in making medical decisions, such as whether to vaccinate than verbatim information (
Reyna et al., 2021). These posts were aimed at communicating about the risk of COVID-19 in categorical terms, including that the harms of COVID-19 could be severe and that the risks of contracting COVID-19 were substantial (Reyna et al., 2011;
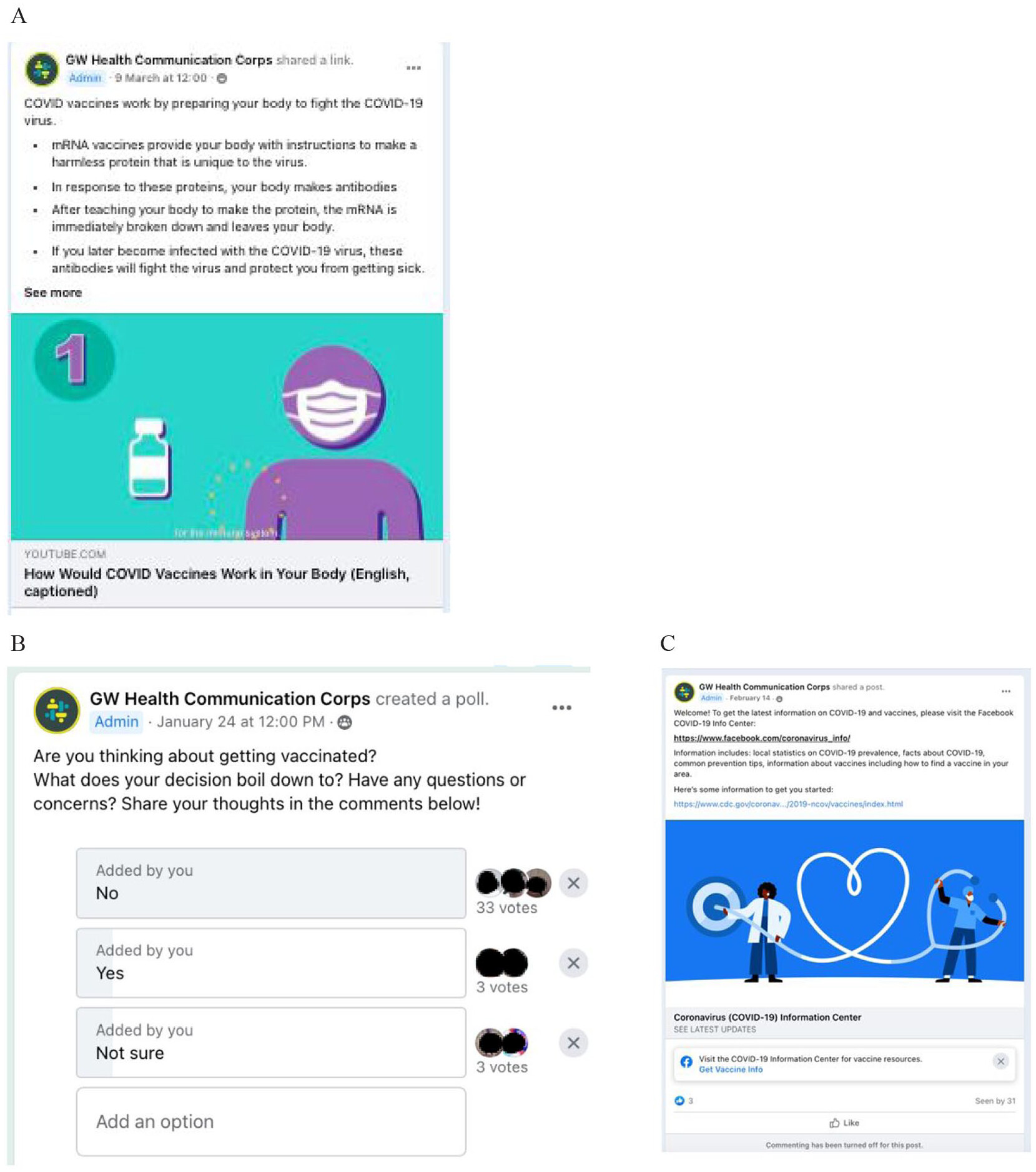
Reyna et al., 2021). For posts about the COVID-19 vaccine, posts were aimed at communicating that the vaccine was a safe and effective response to the threat of COVID-19, that is, that the vaccinated individuals were less likely to contract the disease, that when they did so, their cases were less severe, and that side effects from the vaccine were both less likely and less severe than the risks of infection from the virus (see, e.g.,
Figure 2A). While self-efficacy was covered (e.g., information on finding a site to get vaccinated), this construct was less emphasized, as by this point (late 2021–early 2022), vaccination access had become widespread.
In addition to communicating about the risk of COVID-19 and about the safety and efficacy of vaccines according to Fuzzy Trace Theory, we also developed content aimed at empathically engaging participants and building trust. This was done because prior research indicates that empathetic engagement offers a way to build trust, which in turn can be the foundation of attitude change around disease risks and vaccination (
Larson & Broniatowski, 2021a;
Larson et al., 2018).
To this end, participants were welcomed to the group by asking them to introduce themselves to the group, “Welcome! This group is designed to provide information about COVID-19 vaccines in a non-judgmental space . . .” Group rules promoted being respectful of others, prohibiting bullying, and not sharing misinformation. To elicit concerns, weekly polls were conducted with participants asking them about their intention to vaccinate and reasons for or for not doing so (see
Figure 2B). In addition, participants were given a weekly multiple-choice quiz. For Wave 1, participants were able to comment, post, and direct message moderators. For Wave 2, one of the two intervention groups could not initiate posts, but content otherwise remained the same.
In addition, moderators were trained to address comments and questions in a way that was empathic and respectful. They were told to first thank the participant for their comment and acknowledge their concern as legitimate. Then, they were trained to provide technical information that answered the question or addressed the comment, and then, where possible, to end the response by reiterating the gist that COVID-19 is dangerous, and vaccines are safe and effective (according to Fuzzy Trace Theory). Moderators were on a schedule, so that, one moderator checked in on the group at least daily, and responses to comments were generally made within 24 hours of participants posting them.
Control Group
Participants in the control group were shown a single post that welcomed them and referred them to Facebook’s COVID-19 Information Center. This resource was chosen to simulate usual care on Facebook where the COVID-19 Information Center is the resource for anyone inquiring about COVID or posting about COVID. Posting and commenting features of the control group were disabled as this group was not moderated (see
Figure 2C).
Measures
Sociodemographic factors included: age, gender, race/ethnicity (White, Black, Asian, Hispanic, other); educational attainment (< high school, college degree [or other post high school training], ≥ college degree); household income (U.S. dollars); employment status (employed, other); relationship status (married/living with partner, other); political views (conservative, moderate, liberal); and experience with COVID-19 (e.g., knew someone who got COVID-19).
Primary outcomes were COVID-19 vaccine uptake, intention to get vaccinated for COVID-19, and intention to recommend the COVID-19 vaccine to others. For COVID-19 vaccine uptake, participants were asked, “Since joining this study, have you been vaccinated for COVID-19?” Participants who indicated that they had received at least one vaccine shot were coded as vaccinated. Intention to vaccinate for COVID-19 was measured on a scale from 1 (not at all likely) to 7 (extremely likely) with participants rating their likelihood of getting a COVID-19 vaccine in the next month. Vaccinated participants were imputed as having an 8 on the scale. Participants were also asked about their intention to encourage others (e.g., friend, coworker or family member) to get the COVID-19 vaccine on the same scale.
Secondary outcomes included several other variables related to COVID-19 beliefs and attitudes, as well as those related to vaccines generally speaking. Similar to
Quinn et al. (2019), beliefs were assessed across four dimensions: confidence, complacency, convenience, and trust. COVID-19 confidence is an average of two items which were assessed on a scale from 1 (not at all) to 5 (completely): how much they thought the COVID-19 vaccine was (1) safe and (2) effective. COVID-19 complacency is an average of two items which were assessed on a scale from 1 (not at all) to 5 (completely): how much they thought the COVID-19 vaccine was (1) necessary and (2) important. COVID-19 convenience is an average of two items which were assessed on a scale from 1 (not at all) to 5 (completely): how much they thought the COVID-19 vaccine was (1) convenient and (2) affordable. Trust was one item that assessed on a scale from 1 (not at all) to 5 (completely): how much they trusted the COVID-19 vaccine. General vaccine confidence is an adapted measure of COVID-19 confidence but applied to vaccines generally speaking (e.g., I think vaccines are safe; I think vaccines are effective). Responsibility for vaccination to others is a scale of three items that were adapted from a “gist principles” scale developed in prior work (
Reyna et al., 2011) and summed. It was measured (yes/no) with questions assessing whether a person has a responsibility to (a) myself, (b) the ones I love, and (c) to my community to get vaccinated. In addition, a post hoc measure was developed that differentiated between those who improved in their intention to vaccinate for COVID-19 between baseline and 6 weeks of follow-up. For this variable, scores on intention to vaccinate for COVID-19 were dichotomized into those who improved (e.g., score moved in a positive direction at follow-up) versus those who stayed the same or declined between baseline and 6 weeks.
In addition, to measure engagement with the intervention, participant engagement with the Facebook group was tabulated for the intervention group participants. The total number of times each participant posted, voted on a poll, commented, and liked/gave other type of reaction to a post or comment was tabulated.
Analyses
First, descriptive analyses were conducted to characterize participants overall and by assigned group and wave. Because pre- and post-test outcomes were measured on different scales and observed to be highly non-normal on continuous measures, z-scores for these variables were transformed using either a Box–Cox or rank transformation. For each outcome at 6 weeks, group differences on transformed scores were tested with analysis of covariance (ANCOVA) controlling for the baseline score and wave. For each ANCOVA test, the homogeneity of slope assumption was tested through the baseline x group interaction test, and residuals were examined for approximate consistency with the normality assumption. For categorical variables (i.e., vaccination, improvement in intention to vaccinate), a chi-square test was used to compare differences between groups. The interaction of demographic variables, baseline attitudes to vaccination, and political views were also tested for their effect on the effectiveness of the intervention. Because Wave 1 and 2 study conditions were nearly identical in structure (but differences in group size), differences in outcomes across these waves were tested through a two-way analysis of variance to determine whether it was reasonable to pool the waves and therefore increase statistical power. The results showed effects were similar across waves. There was no wave by treatment group effect. Therefore, the data were pooled.
Results
Across Waves 1 and 2, 478 participants were enrolled in the trial, with 263 assigned to intervention across three Facebook groups and 215 to control across two Facebook groups. The follow-up rate at 6 weeks was 84.3%, with similar rates for both intervention and control (85.6% for intervention and 82.7% for control). There were no significant differences in baseline characteristics between participants who completed follow-up and those who did not.
Mean age of participants was 36.9 years (
SD = 9.7). Participants were predominantly female (74.3%), White (79.9%), and had completed at least some college (78.3%) (see
Table 1). The largest political segment was among conservatives (43.5%). As this was a national sample, participants lived in many states with the most representation from Florida (10.5%), Texas (7.5%), Pennsylvania (7.1%), and California (6.1%). Participants had personal experience with COVID with 28.8% having had COVID themselves, 89.7% knowing someone who was diagnosed, 47.9% knowing someone who was hospitalized, and 34.3% knowing someone who had died of COVID. Participants expressed the following top reasons for not vaccinating: concerns about safety (73.8%); concerns about vaccine effectiveness (67.6%), not trusting the government or pharmaceutical companies (55.2%), having the right to choose (49.6%), and concerns about putting something foreign in their body (40.2%).
Treatment retention rates in the assigned Facebook groups was high with vast majority of participants remaining in their assigned treatment at the end of the 28-day treatment period (intervention = 91.0%, control = 96.5%). On average, participants in the intervention group engaged with content (e.g., commented, reacted) 11.8 times (SD = 25.5) over the course of the intervention. On average, they commented 4.1 times (SD = 12.6), reacted 6.3 times (SD = 15.0), and voted in polls 1.4 times (SD = 2.09). At 6 weeks, 74.7% of participants in the intervention group reported being satisfied or highly satisfied with the program and 76.1% found the messages informative or highly informative.
At 6 weeks, 19 intervention group participants (7.2%) compared with 10 from control (4.7%) reported getting vaccinated for COVID-19 (risk ratio [RR] = 1.5, 95% confidence interval [CI] = 0.74–3.27,
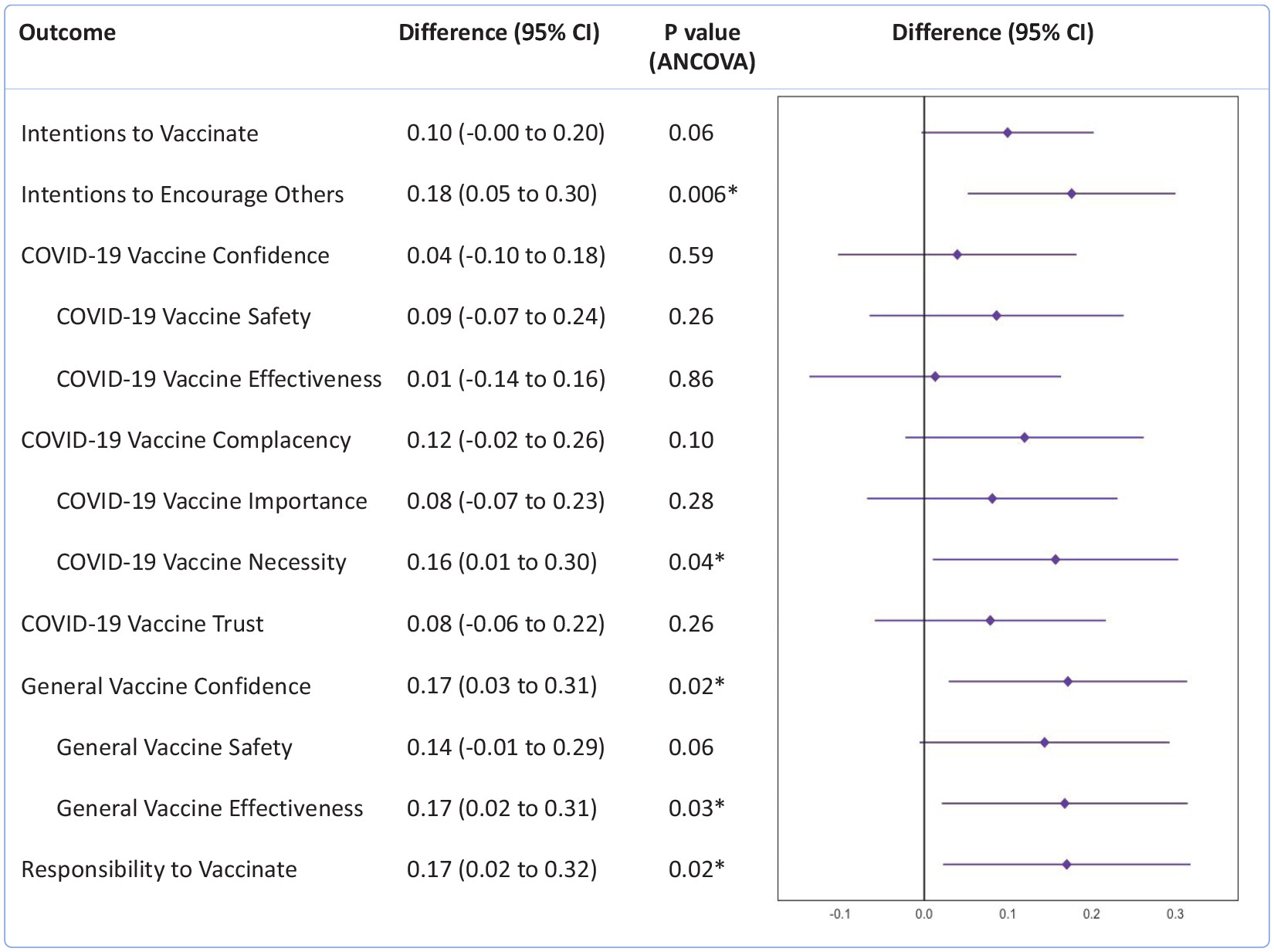
p = .24), a difference that was not significant. The differences between intervention and control groups in intention to vaccinate were not statistically significant though approached significance (
M = 0.10, 95% CI = −0.00 to 0.20,
p = .06). Intervention group members were significantly more likely to intend to encourage others to vaccinate for COVID-19 (
M = 0.18, 95% CI = 0.05−0.30,
p = .006) compared with the control (see
Figure 3). There were no significant differences in COVID-19 vaccine confidence (
M = 0.04, 95% CI = −0.10 to 0.18,
p = .59), COVID-19 vaccine trust (
M = 0.08, 95% CI = −0.07 to 0.23,
p = .26) or COVID-19 vaccine complacency overall (
M = 0.12, 95% CI = −0.02 to 0.26,
p = .10), though participants randomized to the intervention group were more likely to support COVID-19 vaccine necessity (
M = 0.16, 95% CI = 0.01−0.30,
p = .04). General vaccine confidence (
M = 0.17, 95% CI = 0.03−0.31,
p = .02) and responsibility to vaccinate (
M = 0.17, 95% CI = 0.02−0.32,
p = .02) were higher in the intervention condition. Participants in the treatment group were more likely to improve in their intentions to vaccinate for COVID-19 (vs. stay the same or decline) than those in the control. Seventy-five (33.3%) participants in the intervention group and 42 (23.6%) participants in the control group improved in their COVID-19 vaccination intentions (RR = 1.4, 95% CI = 1.02, 1.95,
p = .03). Among demographic and COVID experience variables tested for an interaction on intervention effect, none of the variables was significant.
Discussion
The COVID-19 vaccination rollout and the spread of misinformation about COVID-19 and COVID-19 vaccines on social media have created an urgent need to develop and test interventions on social media that address vaccine hesitancy (
Limaye et al., 2021). This study of unvaccinated individuals conducted approximately 1 year after COVID-19 vaccines became widely available—during the peak of the Omicron variant wave in the United States and almost 2 years after the start of the pandemic—sought to understand whether moderated private Facebook groups that discussed COVID-19 vaccines could provide information on COVID-19 vaccines and shift participants’ intention to vaccinate and vaccination.
Small positive findings were found for some of the primary and secondary outcome variables. Improvements were found for beliefs related to the importance of encouraging others to get vaccinated, the need for COVID-19 vaccination, general vaccine confidence and the responsibility to vaccinate. Participants in the treatment group were also found to be more likely to improve in their intentions to vaccinate for COVID-19 (vs. stay the same or decline) than those in the control. However, despite these positive findings, changes in vaccination rates or intention to get vaccinated for COVID-19 during the 6-week study missed statistical significance at the p < .05 level. Also, other key vaccine-related beliefs, including COVID-19 intention to vaccinate, COVID-19 vaccine confidence (including safety and efficacy) and COVID-19 vaccine trust, showed no statistically significant intervention effects. These mixed findings indicate that this population may require additional efforts to have more positive changes in COVID-19 vaccine-related beliefs and intentions.
The lack of positive findings for all primary outcomes may be the result of the timing of the study which was almost 2 years into the start of the pandemic. By this point, the pandemic had changed as the virulent Delta variant of COVID-19 was waning and the milder Omicron variant was taking off which may have led to perceptions of COVID-19 as mild and non-threatening. Indeed, we found that, as expected, prior to joining the groups, the majority of participants did not believe that COVID was a threat and expressed concerns about the safety of vaccines and their effectiveness, as well as having a high level of distrust of the government and/or pharmaceutical industry. This may have been true especially for those who were politically moderate or conservative as those individuals appeared to have more entrenched views about vaccines. By this point in the pandemic, our empathic approach to engagement was not able to change beliefs and attitudes of some participants.
In addition, stigma associated with vaccination in some vaccine-hesitant communities may have compelled individuals to inaccurately report their own vaccine intentions (
Miller, 1985). Consistent with this explanation, while participants did not shift on some beliefs, they did shift on others specifically related to the responsibility of others. This may also indicate that people with entrenched views may be more likely to consider new points of view for people other than themselves, and this may be an important step leverage point in moving to change their own beliefs (
Bauer, 1964;
Dane, 2010), potentially reflecting the importance of appeals to influence others and the larger social benefit in promoting vaccination (
Chou & Budenz, 2020).
This study represents a novel application of social media. While prior randomized trials of social media around vaccination had largely made use of factual corrections and/or Facebook simulations (e.g., exposing participants to mock-ups of Facebook pages and comments (
Daley et al., 2018;
Kim et al., 2020), we demonstrated that a COVID-19 vaccine intervention could be delivered in the real-world setting of Facebook groups and evaluated. This is important as Facebook and other social media have become a key setting where many people spend their leisure time and get health information (
González-Padilla & Tortolero-Blanco, 2020;
Rosenberg et al., 2020); it is therefore important to develop and test interventions in these settings. Other enhancements to our intervention for future trials might include individualized components (e.g., tailored messaging), as well as variations in messaging strategy (e.g., comparisons of gist vs. verbatim framing).
While we did not find change across all measures, we nonetheless found that moderated groups on Facebook were overall highly acceptable to participants at enrollment. The vast majority of participants in both groups remained in the groups for the duration of the trial and, for the intervention group, reported high levels of satisfaction with the intervention. While engagement and satisfaction were high, running the groups was challenging for moderators and did require constant attention from them. Initially, participants were given the option of posting, as well as commenting on existing posts. This feature was disabled in Wave 2 as we came to recognize that doing so allowed participants the ability to steer conversations in counter-productive directions, including sometimes promoting conspiracy theories and sensationalized stories of vaccine harms. Future studies may seek to better understand how group architecture features (e.g., permissions for posting) should be manipulated for health education around controversial topics.
Strengths and Limitations
The strengths of this study are that it represents one of the first studies to explore how social media private groups can be used for the promotion of COVID-19 vaccine uptake. This study is strengthened by being anchored to a real-world setting, Facebook, which could make scaling such groups feasible. The participants enrolled in the study were not seeking information about vaccines and therefore may be more likely to be representative of vaccine-hesitant individuals.
The limitations of this study are those associated with MTurk and online recruitment. Though we implemented several fraud reduction procedures, some participants could have lied about their vaccination status to collect gift cards. In addition, our study period of 6 months was short which meant that we did not have time to pilot test such variables as optimal group size and content moderation strategies and that our follow-up period was short. Based on lessons learned in Wave 1, we therefore recruited smaller group sizes and adopted stricter content moderation policies for Wave 2. We recommend that future studies deliberately test out variations in group size, intervention length, content moderation strategies, and theoretically motivated messaging strategies, as they may affect targeted outcomes, as well as design longer periods of follow-up. In addition, our study was conducted well into the pandemic. Future studies may wish to investigate whether vaccine-related beliefs and attitudes are more malleable closer to the time that a new vaccine or treatment is being introduced.
Conclusion
In conclusion, empathic, gist-based messages, when delivered in private groups on social media platforms like Facebook can influence some COVID-19 vaccine-related intentions, attitudes, and beliefs. Future areas of examination can include manipulating messaging strategies, such as group size and source of message, as well as determining whether additional outreach strategies can further improve vaccine intentions and vaccination.
Acknowledgments
The authors acknowledge and thank Nathan Lu and Neel Bhagwat for their help with message design, group moderation, and data collection.
Ethics Approvals
Institutional Review Board approvals were obtained from George Washington University.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.A. receives royalties for the sale of Text2Quit. DAB has received consulting fees from Merck & Co. for participating in the 2021 Merck Global Vaccine Confidence Expert Input Forum, and has received a speaking honorarium from the United Nations Shot@Life Foundation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vaccine Confidence Fund (MPIs: Broniatowski, Abroms).