“Ms. Adams noticed that he attempts to spin practically all materials that are presented to him—crayons used for art projects, rocks on the playground, balls at gym.”
Paige just turned 3 years old and recently started attending an inclusive preschool. When Paige entered the room on her first day of school, her body tensed and while standing on her toes, she briefly flapped her arms for 3 to 4 s with her mouth gaped open. At circle time, Ms. Adams, Paige’s teacher, allowed her to choose the book they were going to read. When Ms. Adams took the book, Paige’s body tensed and she repeated the flapping behavior. Ms. Adams noticed this repetitive behavior throughout the day, especially when Paige was excited. The episodes were brief and did not seem to interrupt Paige’s ability to participate in class activities.
Cole is a 5-year-old boy who is also in Ms. Adams’s class. At music time, Cole chose the maracas. Although most of the other students attempted to play their musical instruments along with the song, Cole spun his maracas on the ground with his head cocked to the side. When the paraeducator stopped the spinning maracas and tried to help Cole shake them, Cole screamed and threw himself to the ground. Ms. Adams noticed that he attempts to spin practically all materials that are presented to him—crayons used for art projects, rocks on the playground, balls at gym. If she did not forcibly stop Cole from spinning toys, he would likely spin objects all day and not participate in any class activity or interact with his classmates.
Many teachers and parents of young children with disabilities, particularly autism spectrum disorder (ASD), are familiar with young children who engage in repetitive and restrictive behaviors such as flapping, spinning, and rocking. This type of restrictive and repetitive behavior, or stereotypy, can be common, over time it can become problematic or more intensive. Stereotypy needs to be evaluated as a challenging behavior if it is interfering with learning/living skills or is dangerous. The Division for Early Childhood (DEC) of the Council for Exceptional Children’s Recommended Practices (A4) guide practitioners to conduct assessment that include all areas of development and behavior to learn about the child’s strengths, needs, preferences, and interests (
DEC, 2014).
In this article, we provide information that parents and practitioners can use to help them decide whether and when stereotypy requires intervention along with strategies that can possibly decrease the rate of stereotypic behavior to minimize interference with living/learning skills, social acceptance and injury.

What Is Stereotypy?
Stereotypy is the broad term used to describe rigid, invariant, repetitive body movements or movement of objects (
Matson & Nebel-Schwalm, 2007). Practitioners and parents may be more familiar with the term self-stimulatory behavior or “stimming” because it is often thought that the individual engages in the behavior to gain sensory input. Although this is true, for some the behavior may occur over time because the child has received a social consequence, such as gaining attention, escaping, or avoiding an undesirable activity or getting access to a tangible item/activity. (See
Table 1 for examples of stereotypic behavior and perceived function.) Because the same behavior can serve different functions, the broader term stereotypy will be used throughout this article.
“Practitioners and parents may be more familiar with the term self-stimulatory behavior or “stimming”…
When Does Stereotypy Require Intervention?
Repetitive movements are common in typical early childhood development (
Leekham, Nieto, Libby, Wing, & Gould, 2007) and the sensory input that the child receives through these repetitive actions is important for nervous system and motor development.
“Stereotypic behaviors usually subside by the age of 3 years.”
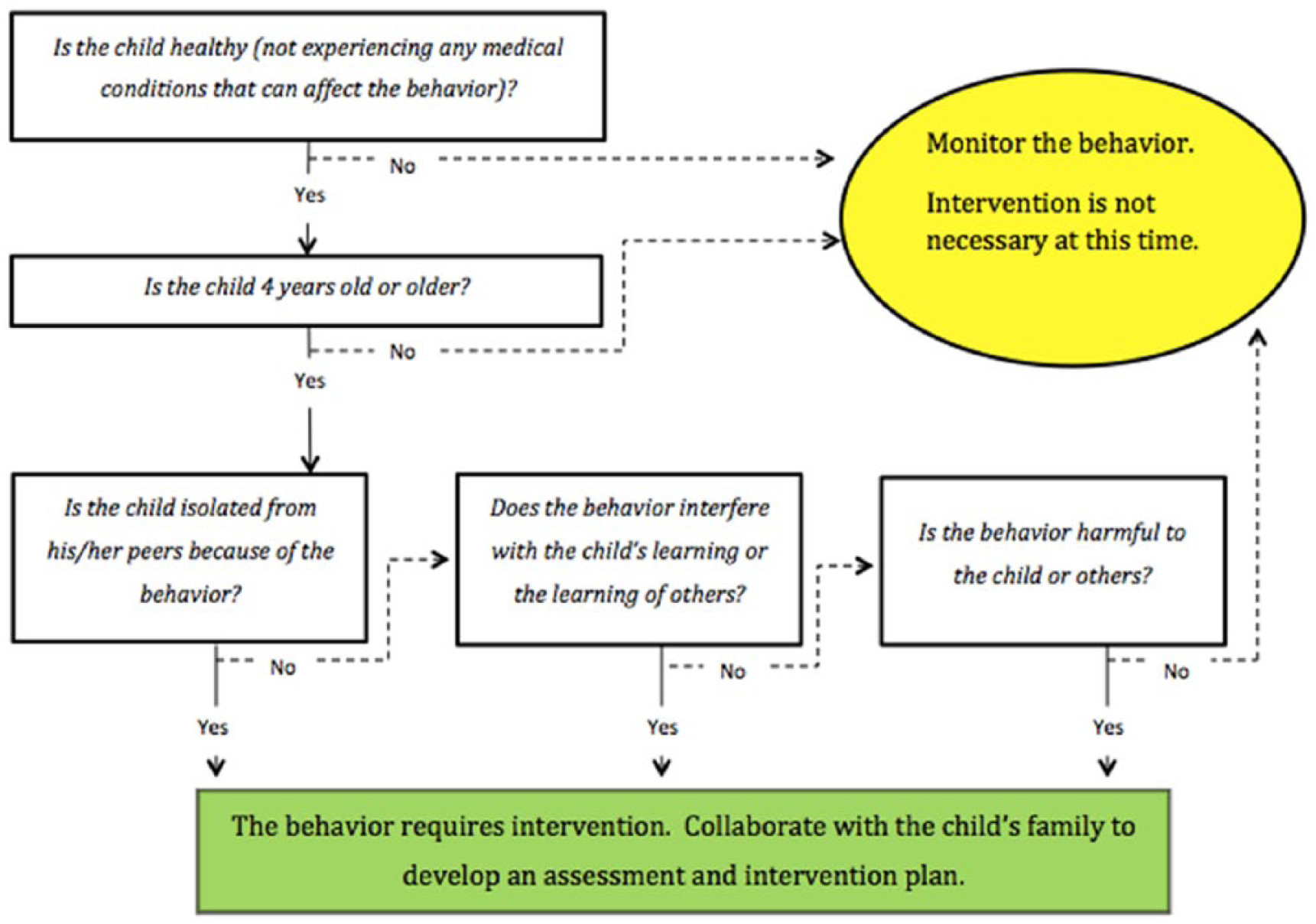
Because stereotypy is part of typical development, it is important to first determine whether the stereotypy requires intervention (see
Figure 1 for a decision making guide). This decision should be based on a number of factors including age, disability, function, and family priorities. It is also important to consider the form and the context of the behavior as well as how limiting and stigmatizing the stereotypy appears to be.
When deciding whether a child’s stereotypic behavior requires intervention, parents and practitioners should consider their responses to the following questions:
Does the Child Have a Possible Medical Condition That Can Affect the Behavior?
Stereotypies may increase with illness, and self-injurious behaviors have been shown to increase with physical discomfort, such as in children with intellectual disabilities who have ear infections (
Carr & Smith, 1995). If the child has a medical condition that affects behavior, it should be addressed first through medical interventions before behavioral supports are deployed.
How Old Is the Child?
Stereotypic behaviors usually subside by the age of 3 years. Teachers generally show greater concern if these behaviors persist past 3 years of age because the behaviors may interfere with child’s ability to learn new adaptive skills (
Matson & Nebel-Schwalm, 2007). However, if the child is below 3 years of age, the intensity, frequency, and other challenges the stereotypy may bring should be considered.
“The team decides that his repetitive object spinning must be addressed because it occurs frequently and for long durations, preventing him from participating in class and interacting with others.”
Is the Child Isolated From His or Her Peers Because of the Behavior?
There is a great deal of social discrimination against those who display stereotypy (
Jones, Wint, & Ellis, 1990). Children who engage in high rates of stereotypic behavior may have limited opportunities to participate in social activities if their peers react negatively to the behavior.
Does the Behavior Interfere With the Child’s Learning or Others’ Learning?
If the child’s behavior is intense or frequent, it may interfere with the child’s ability to learn by observing others (
Matson & Nebel-Schwalm, 2007), hinder the development of play skills (
Powell, Dunlap, & Fox, 2006), and reduce participation in academic tasks (
Sigafoos, Arthur, & O’Reilly, 2003). Parents and educators should be equally concerned if a child’s behavior disrupts classroom activities and affects other children’s ability to learn.
Is the Behavior Harmful to the Child or Others?
Behaviors that occur at extremely high rates may cause harm, such as repetitive head banging or head butting, require immediate intervention. Data should be collected on intensity and frequency of stereotypy and how often it is occurring so practitioners can intervene before increased injury occurs. If self-injury occurs, it is imperative that the practitioners and family prevent the behaviors from happening and conduct a functional behavior assessment (FBA) on the self-injurious behaviors.
The educational team and Paige’s parents meet to discuss whether Paige’s behavior (tensing her body while simultaneously standing on her toes and flapping with her mouth gaped open) requires intervention. The team decides they will not intervene given that Paige just turned 3 years, and the behavior is brief and does not seem to affect her ability to participate in classroom activities or interact with her classmates. They will record how often it occurs and will reconvene in 3 months to examine the data to ensure the behavior is not worsening or beginning to interfere with her learning or social interactions.
Later that week, the educational team and Cole’s parents meet to discuss Cole’s behavior in class and at home. Many of Cole’s classmates avoid playing near him because he takes toys to spin them. Attempts to stop Cole from spinning a toy lead to increasingly aggressive responses toward himself and those around him. The team decides that his repetitive object spinning must be addressed because it occurs frequently and for long durations, preventing him from participating in class and interacting with others.
“If the behavior is problematic, it is important for practitioners and parents to collaborate to understand why the child is engaging in the behavior and identify possible factors that maintain its occurrence.”
What Can We Do to Help Children With Stereotypic Behavior?
Step 1: Identify the Function of the Behavior
The DEC-recommended practice (INS9) requires practitioners use functional assessment across environments to address challenging behaviors (
DEC, 2014). In addition, practitioners and families should work as a team to systematically and jointly evaluate a child and, if needed, implement interventions (TC2;
DEC, 2014). If the behavior is problematic, it is important for practitioners and parents to collaborate to understand why the child is engaging in the behavior and identify possible factors that maintain its occurrence (
Fettig, Schultz, & Ostrosky, 2013). This is typically done by conducting an FBA, a procedure that consists of reviewing the child’s records and interviewing family members and others who know the child well and have experienced the child engaging in the target behavior (refer to
O’Neill, Horner, Albin, Story, & Sprague, 1990 for questionnaires that are commonly used in FBA). Observations of the child engaging in the target behavior are conducted to gather information on what happens immediately before the target behavior takes place (called antecedents), what the behavior looks like (behavior), and what happens after the behavior (consequences; referred to as
ABC Observations;
Miltenberger, 1997). This information is helpful in identifying factors that are likely to produce the behavior and consequences that may be maintaining the behavior (see
National Professional Development Center on ASDs, n.d., FBA module for additional guidance on conducting FBA).

Some indications that the function of the behavior is to gain sensory input include (a) behaviors that occur continuously if the child is left alone for long periods of time, (b) behaviors that occur repeatedly in the same way when the child is left alone, (c) the child appears to enjoy engaging in the behavior, and (d) the child is calm and seems unaware of anything going on around him or her while engaging in the behavior (
Cooper, Heron, & Heward, 2007). Emerging repetitive behaviors may originate from initially looking to gain or avoid sensory input, and even be part of typical motor development. However, the stereotypic behavior may then become socially mediated over time as the behavior has multiple opportunities to be reinforced as the child gets older (
Kennedy, 2002). We will use Cole’s repetitive object spinning behavior from the opening vignette to illustrate how this can occur:
“When creating a behavior plan for any challenging behavior, it is critical to use prevention strategies, replacement skills, and response strategies.”
The educational team conducted an FBA and concluded, “When presented with a solid object, Cole will spin the object while viewing it from the corner of his eye in order to gain visual input.” The team hypothesized that Cole’s object-spinning was maintained by visual stimulation. The director of the program observed Cole’s class and noticed that whenever Cole would begin to spin crayons, the paraeducator would take them away. In doing so, Cole was no longer able to spin the crayons, but he also was not required to participate in the activity. The program director cautioned that if this continued, he might learn that object-spinning not only provides visual reinforcement but can also be an effective way to avoid participating in a class activity.
The FBA process will allow family and practitioners to develop a hypothesis (i.e., reasonable conclusion) about why the behavior is taking place. If it is suspected that the function of the behavior is to gain sensory input, predictions about the type of sensory input that the child receives when engaging in the stereotypic behavior should also be made based on the FBA. The educational team must develop a sound hypothesis regarding the function of the stereotypic behavior to create a strategic behavior plan.
Step 2: Create a Plan to Address the Behavior
With a sound hypothesis about the function of the stereotypy, parents and educators can create a plan that includes strategies to reduce the behavior through prevention and response techniques while teaching the child another, more appropriate behavior that serves the same function as the stereotypic behavior.
Strategies presented below are suggested for consideration if the function of the stereotypy is maintained by sensory input and
not by social functions. If stereotypy were determined by the FBA to be maintained by social consequences, the interventions recommended are not specific to stereotypy but rather to the function. For recommended interventions for challenging behaviors maintained by social functions, see
Rahn, Coogle, Hanna, and Lewellen (2017).
These strategies are the few that have been studied with children as young as 3 years of age (
Ahearn, Clark, MacDonald, & Chung, 2007). There is a clear need for more research of children below the age of 3 years who exhibit stereotypy. The feasibility of using certain interventions across different environments such as day care and home settings must also be determined. Working with other professionals, particularly occupational therapists, may be helpful.
When creating a behavior plan for any challenging behavior, it is critical to use prevention strategies, replacement skills, and response strategies. Strategies should not be used in isolation because they typically will not maintain a decrease in stereotypy over time.
Prevention strategies
Antecedent interventions involve changing the environment or the stimuli that elicits challenging behavior and have been successfully used to reduce stereotypic behavior in children as young as 6 years of age (
Conroy, Asmus, Sellers, & Ladwig, 2005). An antecedent intervention offers a unique advantage: It may prevent the challenging behavior from ever occurring, thus preventing the need to respond to the behavior. This is particularly important in treating stereotypy because preventing the behavior decreases the opportunities for social consequences that may result in stereotypy gaining additional functions, such as escape from nonpreferred activities (
Richman, 2008). In
Table 2, we provide a summary of benefits and potential drawbacks for each identified antecedent intervention.
“A child could be taught, for example, that when he or she is wearing the bracelet, it is not an appopriate time to engage in stereotypy.”
Replacement skills
The information collected during the FBA should provide parents and practitioners with a sense of when the child is most likely to engage in stereotypy. It is possible to teach the child when he could engage in stereotypy and when he should not (
Conroy et al., 2005).
Visual cue cards
The following are tools to teach a child (a) when it is appropriate to engage in stereotypy, and (b) when it is not acceptable to demonstrate the behavior. Use visual cue cards (e.g., yes/no; red/green) or other concrete items (e.g., tray, boxes, bracelet) to assist the child in discriminating between appropriate and inappropriate times to engage in the behavior (
Gauvreau & Schwartz, 2013). A child could be taught, for example, that when he or she is wearing the bracelet, it is not an appropriate time to engage in stereotypy. Also, a student may be taught that when a certain coloring tray is on his or her desk, he or she does not engage in stereotypy.
Conduct brief instructional sessions with the child by presenting the visual cue or object and explaining the expectations of the card or object. The child should be reminded of the expectations before the child is likely to engage in high rates of the behavior.
At the beginning of the activity, the adult should present the visual cue or object to the child, verbally prompting or pointing to the cue to ensure that the child looks at it. This will help show the child that when the cue is present, he or she should not engage in the stereotypy. When the child does not engage in stereotypy for a set period of time, the child should be provided individualized reinforcement.
“Increasing levels of exercise, play, or other forms of physical activity has been found to decrease stereotypy in some individuals and has been studied in children as young as preschool age.”
If the child engages in stereotypy at an inappropriate time, the adult should redirect the child’s attention to the visual cue and remind him or her that it is not time to engage in the behavior while the cue is present.
Teaching a child when he or she may engage in stereotypy can be difficult and must be taught in incremental stages. If the stereotypic behavior occurs at a high rate, it may be necessary for initial teaching sessions to include shorter “no behavior” periods in which the child will be able to successfully refrain from engaging in stereotypy while the cue is present. The length of “no behavior” periods should gradually be increased.
Increase on-task behavior
The inability to participate in activities because of a stereotypic behavior is a strong factor in deciding that the behavior requires intervention. Researchers have found that providing verbal and gestural prompts to orient a student back to the task increased time on task and decreased stereotypic behaviors (
Symons & Davis, 1994).
MacDuff, Krantz, and McClannahan (1993) used picture activity schedules to help children successfully participate in activities, which resulted in reductions in inappropriate behaviors including stereotypic behavior.
Offer physical activity
Increasing levels of exercise, play, or other forms of physical activity has been found to decrease stereotypy in some individuals (
Allison, Faith, & Franklin, 1995) and has been studied in children as young as preschool age (
McLaughlin, 2010). In this study, stereotypy was measured for the 15 min after recess finished. The duration of effects has been shown to range between 40 min (
Celiberti, Bobo, Kelly, Harris, & Handleman, 1997) and 90 min (
Levinson & Reid, 1993), but the exact effect for young children is unknown. As such, it may be appropriate to incorporate multiple active play sessions into several daily routines.
Enrich the environment
Enriching a child’s environment can be an easy way for practitioners and parents to reduce stereotypic behavior in some children, by providing the same type of reinforcement that is being offered by the stereotypic behavior. It should be emphasized that this strategy is most successful when there is a strong match between the sensory input provided by both the alternative and original stimuli. Please refer to
Table 3, which illustrates an example for how to identify similar stimuli based on the stereotypy’s specific sensory input.
Identify and teach alternative behaviors
Once the educational team makes a hypothesis about the function of the behavior, it is important to identify a more appropriate, alternative behavior that can take the place of stereotypy. These should provide the same sensory reinforcement to the child, but in a more appropriate way (
Neitzel, 2009). The alternative behaviors should also be age appropriate, easily taught to the child, and simple for the child to use/access.
“Response interruption, which requires the adult to physically or verbally interrupt the young child when he or she engages in the stereotypic behavior.”
Step 3: Respond to Stereotypic Behaviors as They Occur
Despite the inclusion of prevention strategies in a child’s behavior plan, it is inevitable that some stereotypic behavior will occur so it is important to have a plan for how to react. There exists ample evidence to suggest that the best ways of handling challenging behavior are indirect.
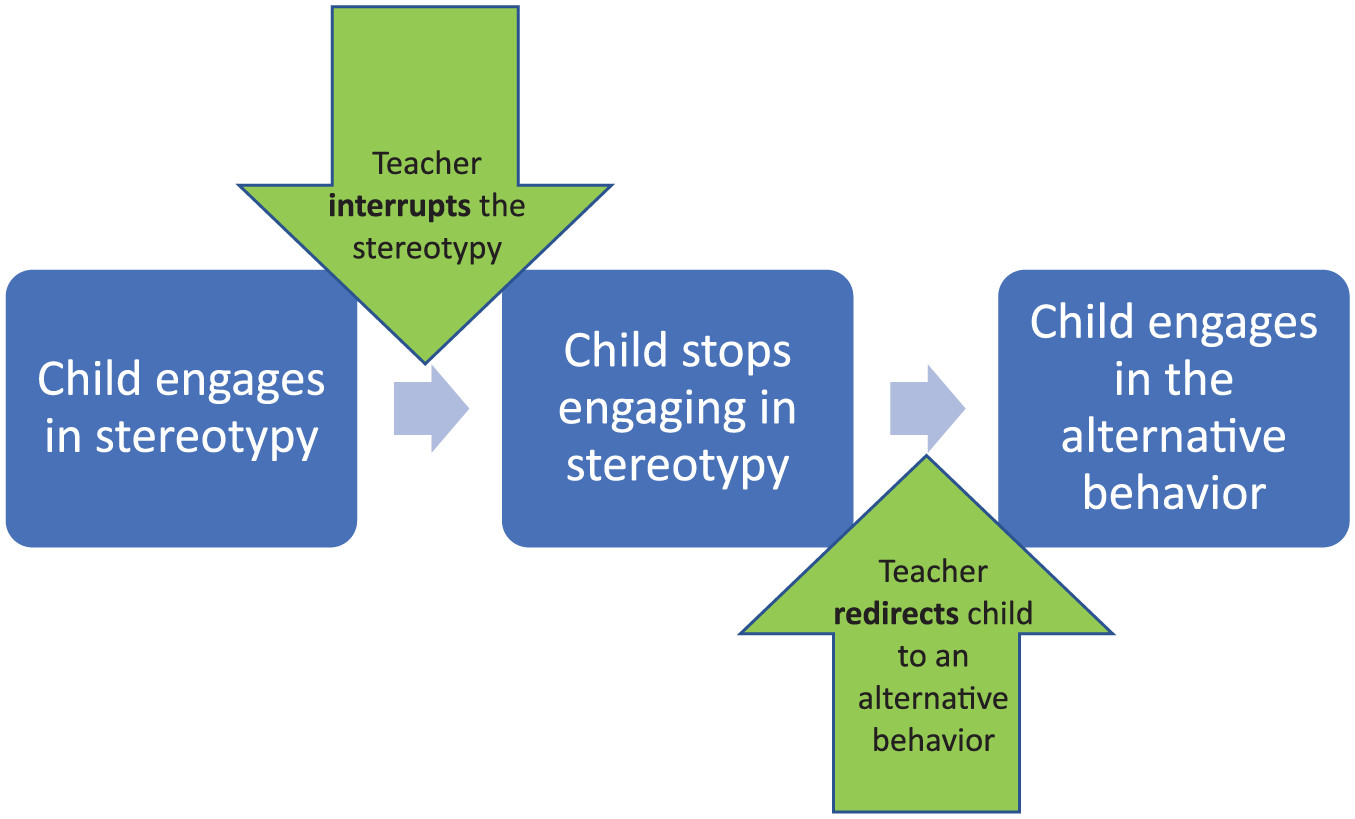
Response interruption and redirection (RIR) techniques, which have been used with children as young as 3 years of age (
Ahearn et al., 2007), involve the adult interrupting the child’s stereotypy and redirecting him or her to engage in the more appropriate, alternative behavior (
Neitzel, 2009). The first component of RIR is to stop the stereotypic behavior so the child does not experience the pleasurable effects of the behavior. In
response blocking, the adult introduces stimuli that can block the intensity of reinforcement that the child would ordinarily receive when engaging in stereotypy (i.e., wear gloves to decrease the tactile effects of hand-clapping; see
Figure 2). A similar procedure is
response interruption, which requires the adult to physically or verbally interrupt the young child while he or she engages in the stereotypic behavior. Both response blocking and response interruption can be used with motor (e.g., hand-flapping) and vocal stereotypies (e.g., humming). For response interruption to be successful, the person giving the demand must be able to elicit compliance from the child; otherwise the young child could simply ignore it.
“No single strategy is effective for all children or behaviors, and that a combination of antecedent, replacement behaviors, and consequence strategies should be included in a child’s behavior plan.”
Response blocking, when used alone in the absence of other behavioral interventions, has been shown to increase aggression. Simply blocking a stereotypic behavior does not teach the child to engage in an appropriate replacement behavior nor provide alternative sensory stimulation, so it is important that it not be used in isolation (
Hagopian & Adelinas, 2001). Accordingly, the second component of RIR is to redirect the child to engage in an appropriate, alternative behavior. Once the teacher blocks the child from engaging in stereotypy, she or he will help the child to perform the selected alternative behavior for a short amount of time and provide immediate reinforcement. As the child begins to use the alternative behavior more often than the stereotypic behavior, teachers can increase the amount of time that is required of the child to engage in the appropriate behavior before receiving reinforcement. See
Figure 3.
Concluding Thoughts
Parents and teachers of young children who engage in stereotypy can use the process outlined in this article to determine if they should intervene. If the decision is made to intervene, the educational team should conduct an FBA to determine the function of the behavior. There are many options of interventions for teachers and parents to use to help the child decrease stereotypy while increasing other more positive skills. The interventions outlined in this article are focused on stereotypy maintained by sensory input. We would like to emphasize that no single strategy is effective for all children or behaviors, and that a combination of antecedent, replacement behaviors, and consequence strategies should be included in a child’s behavior plan (see
Figure 4).
Authors’ Note
Veronica P. Fleury is now affiliated with Florida State University.