

Understanding the menopausal experiences of women with intellectual disabilities: A scoping review
Abstract
Background
Methods
Stage 1: Identifying the research question
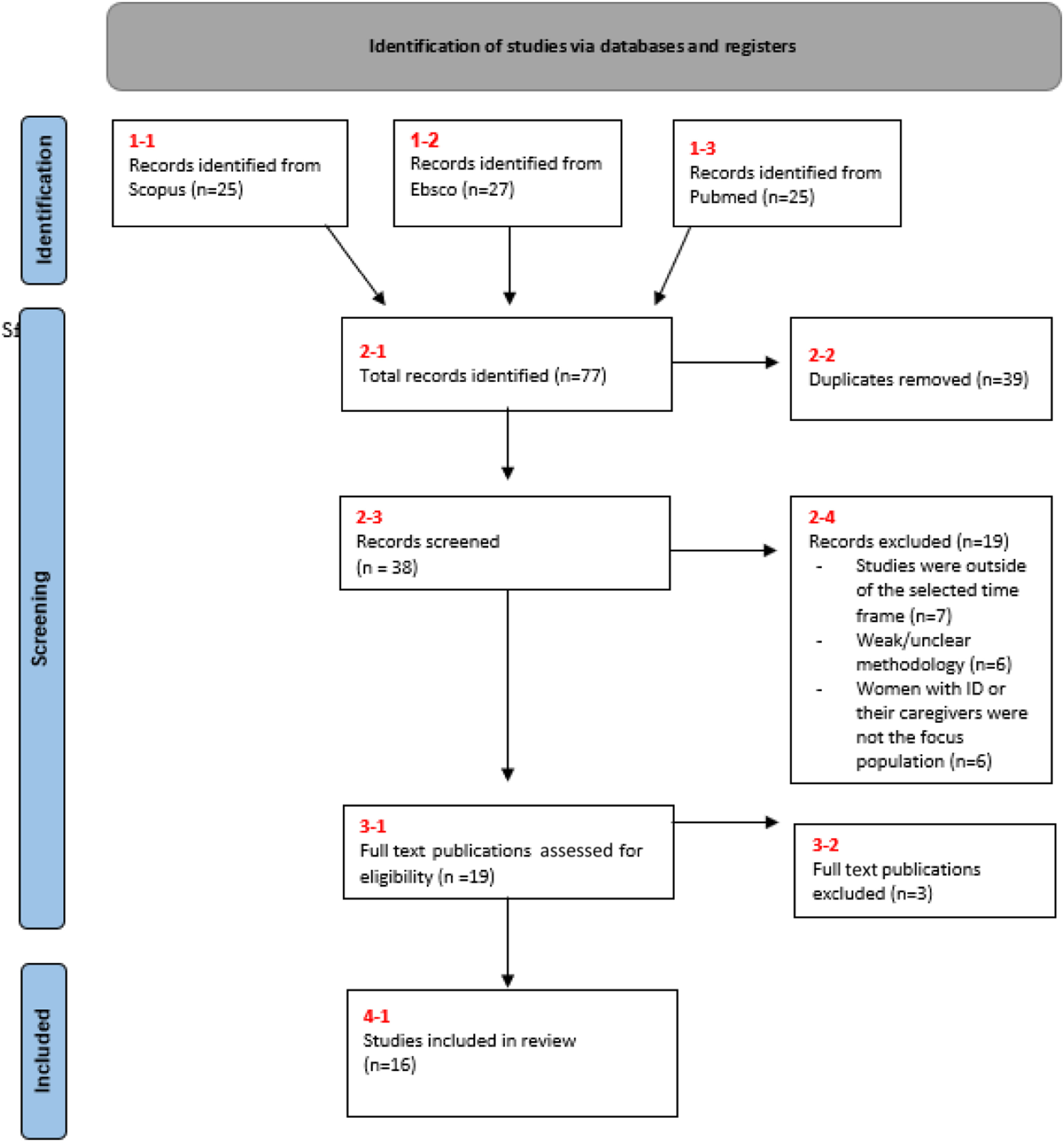
Stage 2: Identifying the relevant studies
Stage 3: Study selection
| Criteria | Determinants |
|---|---|
| Population | Women with intellectual disabilities |
| Formal and informal caregivers of women with intellectual disabilities | |
| Exposure | Peri-menopause |
| Menopause | |
| Post-menopause | |
| Outcomes | Experiences of menopause |
| Knowledge of menopause | |
| Treatment of menopausal symptoms |
Stage 4: Charting the data
Stage 5: Collating, synthesising and reporting the results
| TITLE | Authors | Year | Publication | Context | Methodology | Key findings |
|---|---|---|---|---|---|---|
| REPRODUCTIVE (IN)JUSTICE AND INEQUALITY IN THE LIVES OF WOMEN WITH INTELLECTUAL DISABILITIES IN SCOTLAND | Wiseman, P., Ferrie, J. | 2020 | Scandinavian Journal of Disability Research, 22 (1), pp. 318-329. | Scotland | Open qualitative questionnaire (n=21) and further focus group discussion (3) with 12 women | - Addresses the fact that women with intellectual disabilities are largely absent from mainstream feminist narratives of reproductive justice. |
| HEALTHCARE FOR WOMEN WITH DISABILITIES IN THE CLIMACTERIC AND MENOPAUSE | de Almeida, E.W., Greguol, M. | 2015 | Sexuality and Disability, 33 (2), pp. 279-298. | Global | Narrative literature review | - Despite many of the women in included studies being overweight or having difficulties in performing daily activities most of the study populations perceived their health as being good. |
| - Participants in the studies who were evaluated for level of physical activity were generally classified as being active. | ||||||
| - Women in some studies did not follow the proposed recommendations for routine health checks. | ||||||
| - Reported menopausal symptoms from women were not significantly different from those reported by women in the general population. | ||||||
| MENOPAUSE EXPERIENCES AND ATTITUDES IN WOMEN WITH INTELLECTUAL DISABILITY AND IN THEIR FAMILY CARERS | Chou, Y.-C., Lu, Z.-Y.J., Pu, C.-Y. | 2013 | Journal of Intellectual and Developmental Disability, 38 (2), pp. 114-123. Cited 3 times. | Taiwan | Mixed methods study: a survey performed with women with intellectual disabilities (n=7) and their carers (n=65), semi structured interviews with women with intellectual disabilities (n=4) and their carers (n=10). | - Less than one quarter of the women with intellectual disabilities in the survey had received a gynaecological test while a minority had consulted a GP about menopause. |
| - Women with intellectual disabilities rarely used HRT and lacked access to regular health check-ups. | ||||||
| - Almost all women with intellectual disabilities were not informed by their carers about menopausal issues/symptoms. | ||||||
| - Carers indicated that they did not think it was necessary to prepare women for the menopause. | ||||||
| CAREGIVER AWARENESS OF REPRODUCTIVE HEALTH ISSUES FOR WOMEN WITH INTELLECTUAL DISABILITIES | Lin, L.-P., Lin, P.-Y., Hsu, S.-W., Loh, C.-H., Lin, J.-D., Lai, C.-I., Chien, W.-C., Lin, F.-G. | 2011 | BMC Public Health, 11, art. no. 59, . Cited 14 times. | Welfare institutions in Taiwan. | Cross-sectional, questionnaire-based study (n=1152) from 32 institutions | - Caregivers were familiar with sex education, issues of menopause, and preventive health services but were unfamiliar with issues concerning menstruation in women with intellectual disabilities. |
| - Caregivers in intellectual disability services had a clear role in encouraging women to adopt health practices and to ensure that women accessed primary healthcare. | ||||||
| - Many primary caregivers believed that people with intellectual disabilities lack the capacity to make informed decisions about their sexuality and intimate relationships. | ||||||
| - Parents and staff differed in their attitudes; parents had more conservative views. | ||||||
| - Formal caregiver’s gender, educational level, and experience assisting with reproductive health care were significantly associated in logistic regression analyses with high scores for reproductive health awareness for women with intellectual disabilities. | ||||||
| MENOPAUSAL EXPERIENCES OF WOMEN WITH INTELLECTUAL DISABILITIES | Willis, D.S., Wishart, J.G., Muir, W.J. | 2011 | Journal of Applied Research in Intellectual Disabilities, 24 (1), pp. 74-85. Cited 8 times. | Scotland | Semi-structured interviews with 45 women with intellectual disabilities; (17 Down Syndrome, 28 non-Down Syndrome; age 35–65 years). | - Menopausal experiences of the women with intellectual disabilities and those specifically with Down Syndrome were similar. |
| - The majority of women were unaware of menopause-associated changes in their body. Few women understood why they had menstruated. | ||||||
| - It was difficult for women to understand what changes they experienced were as a direct result of the menopause and what symptoms were as a result of other causes. | ||||||
| - Identified the need for increased training for carers and more tailored resources and health education materials for women with intellectual disabilities. | ||||||
| CARER KNOWLEDGE AND EXPERIENCES WITH MENOPAUSE IN WOMEN WITH INTELLECTUAL DISABILITIES | Willis, D.S., Wishart, J.G., Muir, W.J. | 2010 | Journal of Policy and Practice in Intellectual Disabilities, 7 (1), pp. 42-48. Cited 6 times. | Scotland | Interviews with 69 formal caregivers of 45 women with intellectual disabilities | - Carers reported difficulty separating the psychological and physical consequences of the menopause from behaviours and symptoms arising from other causes. |
| - Carers demonstrated a willingness to talk to women with intellectual disabilities about the menopause and symptoms. This was often approached by discussing personal experiences or those of family and friends. | ||||||
| - Participants were keen to ensure that information they shared was appropriately tailored to the ability level of the individual women they supported. | ||||||
| - Carers acknowledged the need for health resources to be better suited to needs of women with intellectual disability and for more relevant health education training for staff. | ||||||
| A DECADE ON: WHAT HAVE WE LEARNT ABOUT SUPPORTING WOMEN WITH INTELLECTUAL DISABILITIES THROUGH THE MENOPAUSE? | Willis, D.S. | 2008 | Journal of Intellectual Disabilities, 12 (1), pp. 9-23. Cited 4 times. | UK | Semi-structure interviews with 15 women with intellectual disabilities. | - Women with intellectual disabilities had little understanding or knowledge about the menopause. |
| - Women were unable to explain why they had periods and articulated a dislike for and discomfort related to having periods.They expressed feelings of relief and happiness when their periods would stop for good. | ||||||
| - Women felt it was important to take exercise and eat well but had no apparent understanding of eating specific healthy foods. | ||||||
| - Some women reported feeling unhappy with their weight or reported that they were on 'diets' indicating a level of autonomy in their decision about their health. | ||||||
| GOING THROUGH THE MENOPAUSE: PERCEPTIONS AND EXPERIENCES OF WOMEN WITH INTELLECTUAL DISABILITY | McCarthy, M. | 2002 | Journal of Intellectual and Developmental Disability, 27 (4), pp. 281-295. Cited 19 times. | UK | Qualitative element of a larger mixed methods study. Here, findings from interviews with 15 women with intellectual disabilities are reported. | - Levels of knowledge about the menopause was generally low. |
| - Women’s experiences of menopausal changes were predominantly physical. Some emotional aspects were emphasised, but few psychological and social impacts were reported. | ||||||
| - Menopausal changes were presented in the context of other broader age-related issues. | ||||||
| - Most of the women articulated strong preferences for talking only to other women about periods and the menopause. | ||||||
| - Generally, low levels of choice and autonomy were highlighted. | ||||||
| RESPONSES TO WOMEN WITH LEARNING DISABILITIES AS THEY GO THROUGH THE MENOPAUSE | McCarthy, M. | 2002 | Tizard Learning Disability Review, 7 (1), pp. 4-12. Cited 12 times. | UK | Mixed methods study: semi structured interviews with women with learning disabilities (n=30) and questionnaires with 314 GPs in one health district in South East England. | - Relief from menopausal symptoms for women with intellectual disabilities was reported as being unpredictable. |
| - Most GPs lacked comprehensive training to deal with the specific needs of women with intellectual disabilities. | ||||||
| - The impact of menopause in this population was predominantly reported at the physical level. | ||||||
| - Women were likely to need carers who were observant and sensitive to facilitate access to health care services. | ||||||
| - Recommendations suggested it would be beneficial if GPs worked in partnership with the women and their carers. | ||||||
| WOMEN WITH LEARNING DISABILITIES AND THE MENOPAUSE | Martin, D.M., Cassidy, G., Ahmad, F., Martin, M.S. | 2001 | Journal of Learning Disabilities, 5 (2), pp. 121-132. Cited 6 times. | N/A | Narrative review | - Services for people with learning disabilities focused on active sexual health The needs of aging women with intellectual disabilities were often overlooked. |
| - The gynaecological issues of (post-menopausal) women with intellectual disabilities were often compounded by anxieties and fears of gynaecologists. | ||||||
| - Carers of women with intellectual disabilities were more likely to dismiss psychological and physical morbidity among older people with intellectual disability. | ||||||
| - Appropriate health promotion about menopause for women with intellectual disabilities and their carers was recommended. | ||||||
| CAREGIVER ATTITUDES TO GYNAECOLOGICAL HEALTH OF WOMEN WITH INTELLECTUAL DISABILITY | Lin, L.-P., Lin, J.-D., Chu, C.M., Chen, L.-M. | 2011 | Journal of Intellectual and Developmental Disability, 36 (3), pp. 149-155. Cited 4 times. | Taiwan | Cross-sectional study; structured questionnaire survey with caregivers of women with intellectual disabilities recruited using purposive sampling (n=1152). | - Most respondents considered that they were able to provide appropriate advice on menstrual education for the women with intellectual disabilities under their care. |
| - 46% of respondents disagreed or strongly disagreed that the institution should take full responsibility for the provision of education about menstrual issues. | ||||||
| - 37.8% of respondents considered that hysterectomy was an effective way to deal with severe menstrual problems. | ||||||
| - Most of the caregivers were in agreement about the implementation of gynaecological healthcare checks | ||||||
| - 90.1% of the caregivers considered that institutions should limit patients’ freedom in order to avoid sexual problems associated with abandoning contraception use after menopause. | ||||||
| - 84.7% of respondents disagreed or strongly disagreed that symptom relief was unnecessary, while 97.2% agreed or strongly agreed that a healthy lifestyle was more important. | ||||||
| CHINESE WOMEN WITH 29-30 CGG REPEATS HAVE AN EARLIER MENOPAUSE. | Tang, R.; Chen, R.; Luo, M.; Lin, S.; Yu, Q. | 2020 | Climacteric | Beijing, China | Mixed method. Analysis were part of a prospective, open cohort, community-based longitudinal study, the PALM study, which aimed to investigate ovarian aging in midlife women in China. | - The FMR1 CGG repeat sizes might have played a role in the mechanisms of the ovarian aging process and thereby affected the timing of menopause. |
| - Women with 29–30 FMR1 CGG repeats may have experienced menopause approximately 2 years earlier than those carrying 28 or 31 CGG repeats and had a longer FSH fluctuant period. | ||||||
| DISCUSSING THE MENOPAUSE WITH WOMEN WITH LEARNING DISABILITIES. | McCarthy M; Millard L | 2003 | British Journal of Learning Disabilities, 31, 9–17 | UK | The findings reported in the present study are from part of large research project, which had four different phases of data collection, all conducted between 1999 and 2000. Presented in this paper is are results from semi structured interviews describing the issues which arise when talking to women with learning disabilities about the menopause. | - Most women did not know or recognize the commonly used terms related to menopause. It was recommended that these terms need to be explained at an early stage and reminders about terminology should be given. |
| - The use of pictures and other visual resources was strongly recommended. | ||||||
| - It was suggested that workers raising issues of ‘how people’s bodies change as they get older’ need to be sensitive to the fact that women may not want to be seen as older and also to the possibility that such discussion may spark memories of bereavement. | ||||||
| - There appeared to be little role for male staff in directly supporting women with intellectual disabilities. | ||||||
| - Older female staff who share their experiences can help ‘normalize’ the experience of menopause and sensitivity is needed in discussions of how the menopause effects women. | ||||||
| FEMALE CARRIERS OF FRAGILE X PREMUTATION HAVE NO INCREASED RISK FOR ADDITIONAL DISEASES OTHER THAN PREMATURE OVARIAN FAILURE. | Hundscheid RD; Smits AP; Thomas CM; Kiemeney LA; Braat DD | 2003 | American journal of medical genetics. 117A:6–9 (2003). | Netherlands | Involved. 152 women who were premutation carriers and 112 other women (59 with a normal FMR-1 gene and 53 with a full mutation) | - No statistically significant differences in the occurrence of diseases (such as cardiovascular disease and osteoporosis were found to be associated with menopause. |
| - Lower bone mineral density was observed only in women who were premutation carriers but these women were not at increased risk of additional medical problems. | ||||||
| - Carrying the premutation may have affected a womans ovaries but did not significantly increase the risk for additional medical problems. | ||||||
| OBESITY ENHANCES VERBAL MEMORY IN POSTMENOPAUSAL WOMEN WITH DOWN SYNDROME. | Patel BN; Pang D; Stern Y; Silverman W; Kline JK; Mayeux R; Schupf N | 2004 | Neurobiology of Aging 25 (2004) 159–166 | NY, United States | Mixed methods study which: compared the performance of healthy nondemented obese and non-obese women (n=116) with Down Syndrome (DS) on a broad spectrum of cognitive tests and review of clinical assessments. | - Estrone levels were 66.9% higher in obese postmenopausal women than in non-obese postmenopausal women and 136% higher in obese premenopausal women than in non-obese premenopausal women. |
| - Obese postmenopausal women performed significantly better than non-obese women on measures of verbal memory and on an omnibus test of neuropsychological function, but did not differ significantly in verbal fluency, language, praxis or visuospatial functioning. | ||||||
| - Among premenopausal women, there was no difference in cognitive function between obese and non-obese women. | ||||||
| - Obese postmenopausal women with Down Syndrome performed better than both normal weight and overweight women on tests of verbal explicit memory and performed better than normal weight, but not overweight, women on an omnibus test of neuropsychological functioning. | ||||||
| ONSET OF DEMENTIA IS ASSOCIATED WITH AGE AT MENOPAUSE IN WOMEN WITH DOWN'S SYNDROME. | Schupf N; Pang D; Patel BN; Silverman W; Schubert R; Lai F; Kline JK; Stern Y; Ferin M; Tycko B; Mayeux R | 2003 | Annals of Neurology Vol 54 No 4 | NY, United States | Mixed methods. Clinical assessments of postmenopausal women with Down Syndrome, 40 to 60 years of age. Multivariate regression analyses to determine the relation of age at menopause to age at onset of Alzheimer’s disease, | - Women with early onset of menopause (46 years or younger) had earlier onset and increased risk of Alzheimer’s disease (AD) compared with women with onset of menopause after 46 years. |
| - Women with dementia had higher mean serum sex hormone binding globulin levels than women without (86.4 vs 56.6 nmol/L, p 0.02), but similar levels of total estradiol, suggesting that bioavailable estradiol, rather than total estradiol, was associated with dementia. |
Results
Extent of the literature
Characteristics of the literature
Perceptions of general health and healthy living
Knowledge of menstruation and menopause
Menopausal symptoms and bodily changes
Women’s access to health care
Sources of knowledge information and support
Knowledge and attitudes of caregivers and health professionals
Discussion
Considerations for future research
Implication for carers and health care providers
Conclusion
Declaration of conflicting interests
Funding
ORCID iD
Footnotes
References
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In

Keywords
Rights and permissions
Article versions
Authors
Metrics and citations
Metrics
Journals metrics
This article was published in Journal of Intellectual Disabilities.
View All Journal MetricsPublication usage*
Total views and downloads: 6201
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 11 view articles Opens in new tab
Crossref: 13
- Using Network Analysis to Understand the Associations Between Menopausal Symptoms and Mental Health in Women With Intellectual Disabilities
- Disparities in Hormone Replacement Therapy Prescribing for Women With Intellectual Disabilities
- Understanding perimenopause and menopause treatment in women with intellectual disability: a retrospective cohort study
- Exploring menstrual symptom frequency and impact on people with neurodevelopmental conditions
- Menopause as a factor in psychological, behavioural and cognitive changes in women with learning disabilities
- Knowledge and Understanding of Menstrual Health in Women With Intellectual Disabilities: A Brief Report
- The Palgrave Encyclopedia of Disability
- Good Intentions, Poor Execution? Why Current Workplace Policies on Menstrual and Menopausal Health Fall Short
- The Impact of Menopause on the Mental Health of Women With an Intellectual Disability: A Scoping Review
- Lesbian, gay, bisexual, transgender and queer (LGBTQ+) menopause: Literature review, knowledge gaps and research agenda
- View More
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.
