

Exploring the training, implementation and utilisation experiences of lung ultrasound accredited physiotherapists in the United Kingdom: A national survey
Abstract
Background:
Methods:
Results:
Conclusion:
Introduction
Methods
Survey design and development
Survey pilot
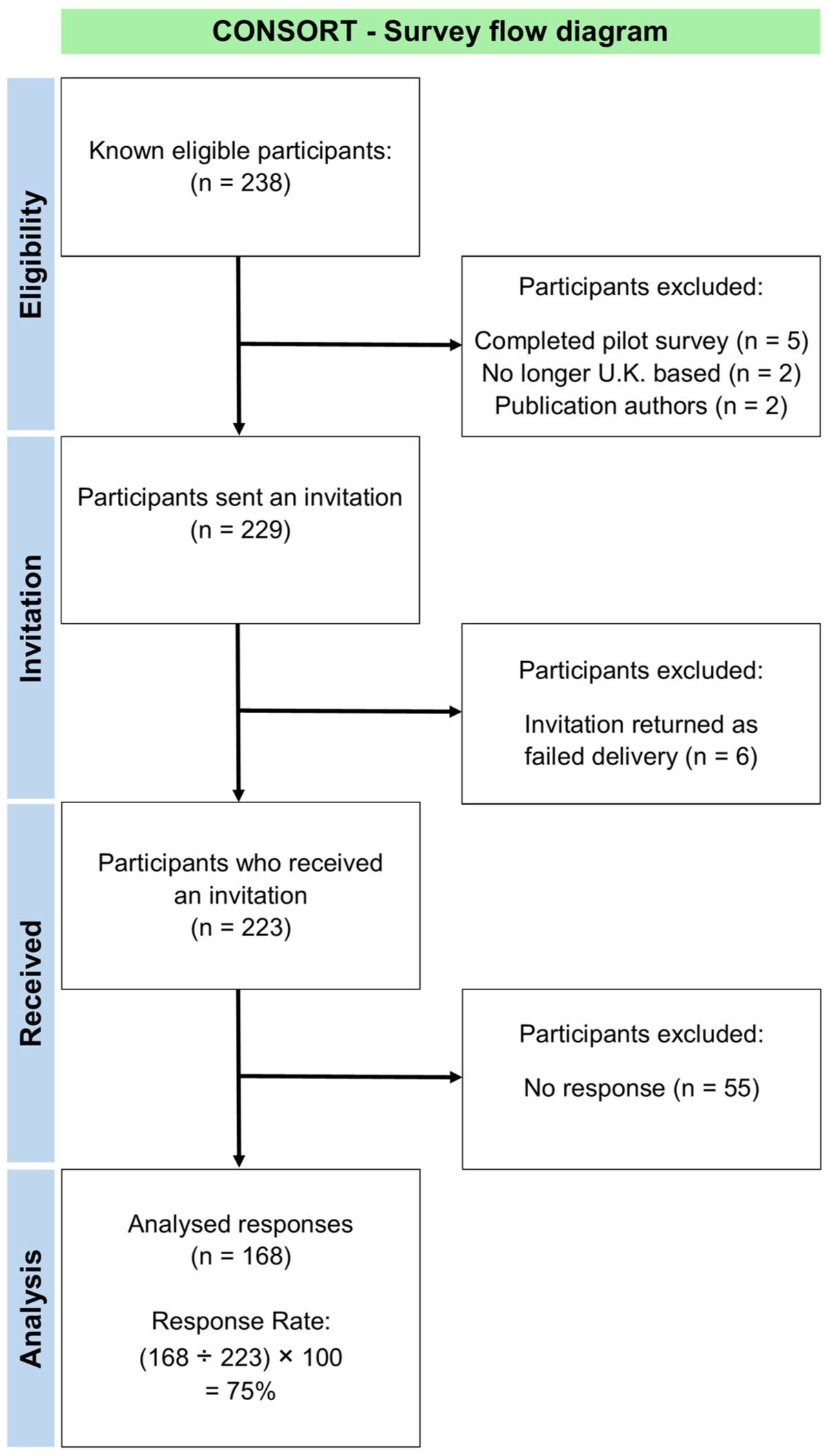
Survey administration
Survey data analysis
Results
| Demographics and characteristics | |||||
| Do you currently use LUS in your physiotherapy practice? | Yes | No | Other | ||
| 92% | 5% | 3% | |||
| What Band were you when you gained your LUS accreditation? (i.e. Band 5 – Graduate, Band 6 – Enhanced level, Band 7 – Advanced level) | Band 5 | Band 6 | Band 7 | Band 8a | Band 8b |
| 0% | 23% | 61% | 14% | 2% | |
| What type of physiotherapy role were you in at the time of gaining your LUS accreditation? | Static role | Respiratory rotational | General rotational | Other | |
| 87% | 9% | 2% | 2% | ||
| Which clinical area(s) do you primarily use your LUS skills in now? | Hyper-acute | Acute | Out-patients | ED | Domiciliary |
| 91% | 44% | 4% | 1% | 1% | |
| Are you an approved LUS mentor/trainer? | Yes | No | Don’t know | ||
| 33% | 64% | 2% | |||
| Accreditation training and mentoring | |||||
| Which LUS training programme did you accredit in? | FUSIC® | CACTUS | FAMUS | BTS | |
| 95% | 4% | 0.5% | 0.5% | ||
| How was your place on any introductory LUS course funded? | Employer | HEE | “In-house” | Other | Self-funding |
| 49% | 15% | 15% | 12% | 10% | |
| How was your LUS module registration fee funded? | Employer | Self-funding | HEE | Other | |
| 48% | 32% | 11% | 9% | ||
| How many different mentors/trainers helped you through your LUS accreditation? | 1 Mentor | 2 Mentors | 3 Mentors | ⩾4 Mentors | |
| 52% | 37% | 9% | 2% | ||
| What profession was your LUS mentor (or mentors) from? | Physio | Doctor | Adv. prac. | Radiologist | CCS |
| 50% | 44% | 4% | 1% | 1% | |
| Did you use remote mentoring during your LUS training? | Yes | No | Don’t know | ||
| 27% | 73% | 0% | |||
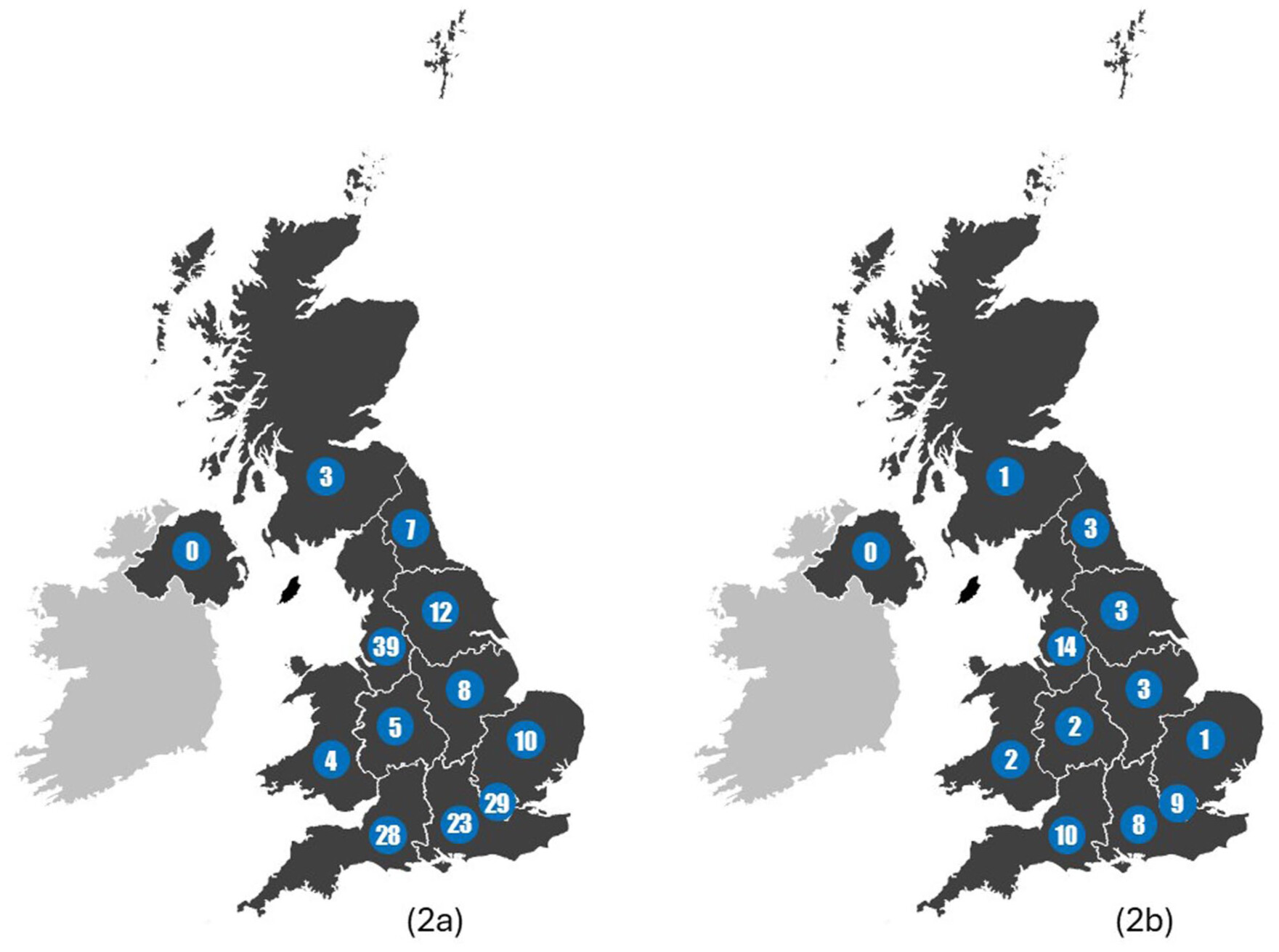
Demographics
LUS accreditation training & mentoring
LUS implementation and governance
| Implementation | |||||
| Do you have consistent access to an ultrasound machine? | Yes | No | Don’t know | ||
| 90% | 10% | 0% | |||
| Do you have a dedicated ultrasound machine for physiotherapists to use for LUS? | Yes | No | Don’t know | ||
| 23% | 77% | 0% | |||
| To date, have you used your LUS skills outside of you contracted working hours in an “on-call” situation? | Yes | No | Not on-call | ||
| 40% | 58% | 2% | |||
| Governance | |||||
| Did you or the wider physiotherapy team need to gain any approvals or permissions from individuals or departments to implement and use LUS? | Yes | No | Don’t know | ||
| 32% | 54% | 14% | |||
| Were you or the wider physiotherapy team asked to create any documents to allow you to implement and use LUS? | Yes | No | Don’t know | ||
| 38% | 52% | 10% | |||
| How are your LUS scan images stored or archived? | US machine | Not stored | Local drive | USB drive | PACS |
| 74% | 7% | 5% | 5% | 4% | |
| How do you report/document your LUS scan findings? | Patient notes | PACS | Clinic letter | Other | |
| 97% | 1% | 1% | 1% | ||
| During the LUS implementation process, were you aware of any factors that negatively impacted progress? | Yes | No | Don’t know | ||
| 26% | 57% | 17% | |||
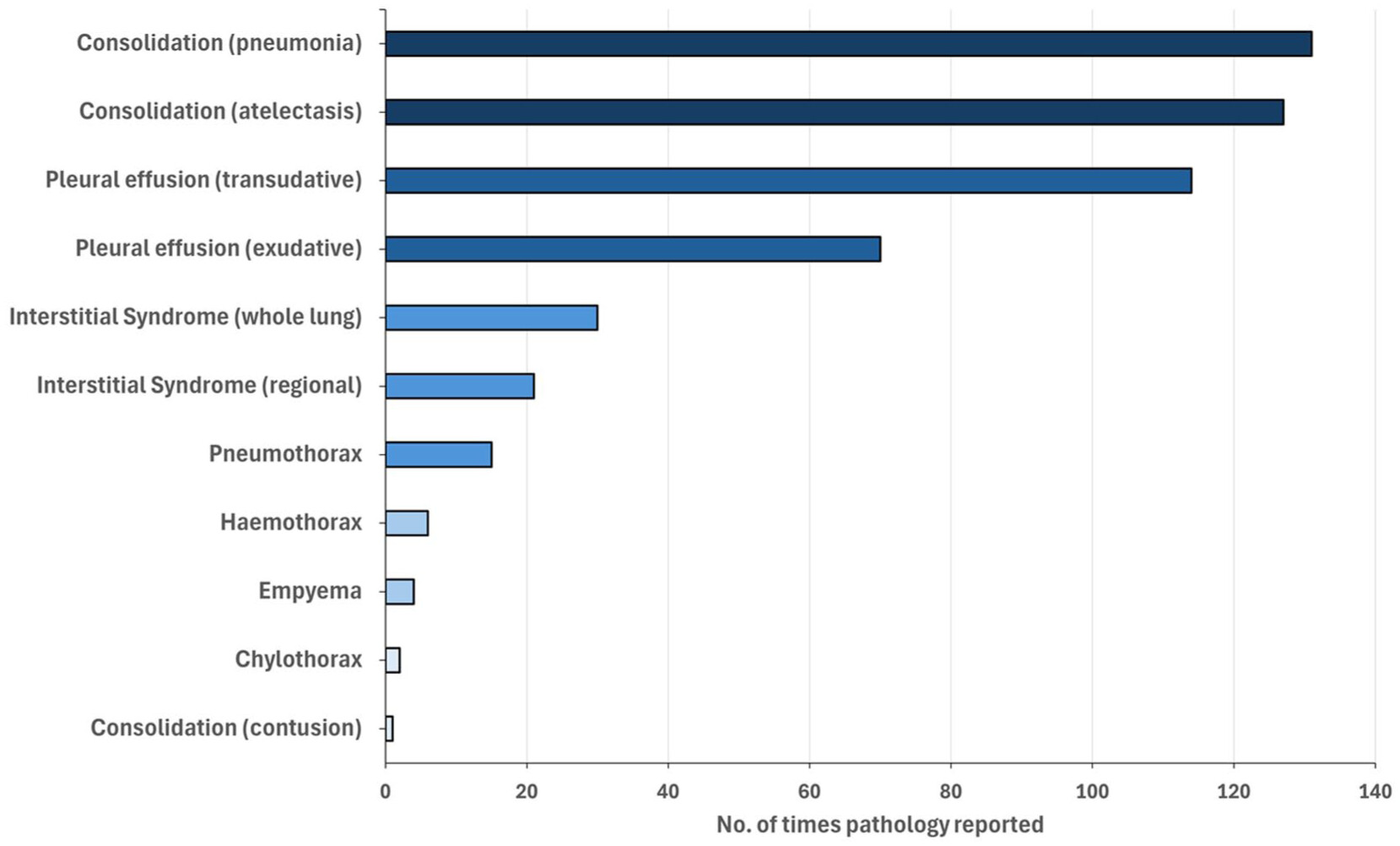
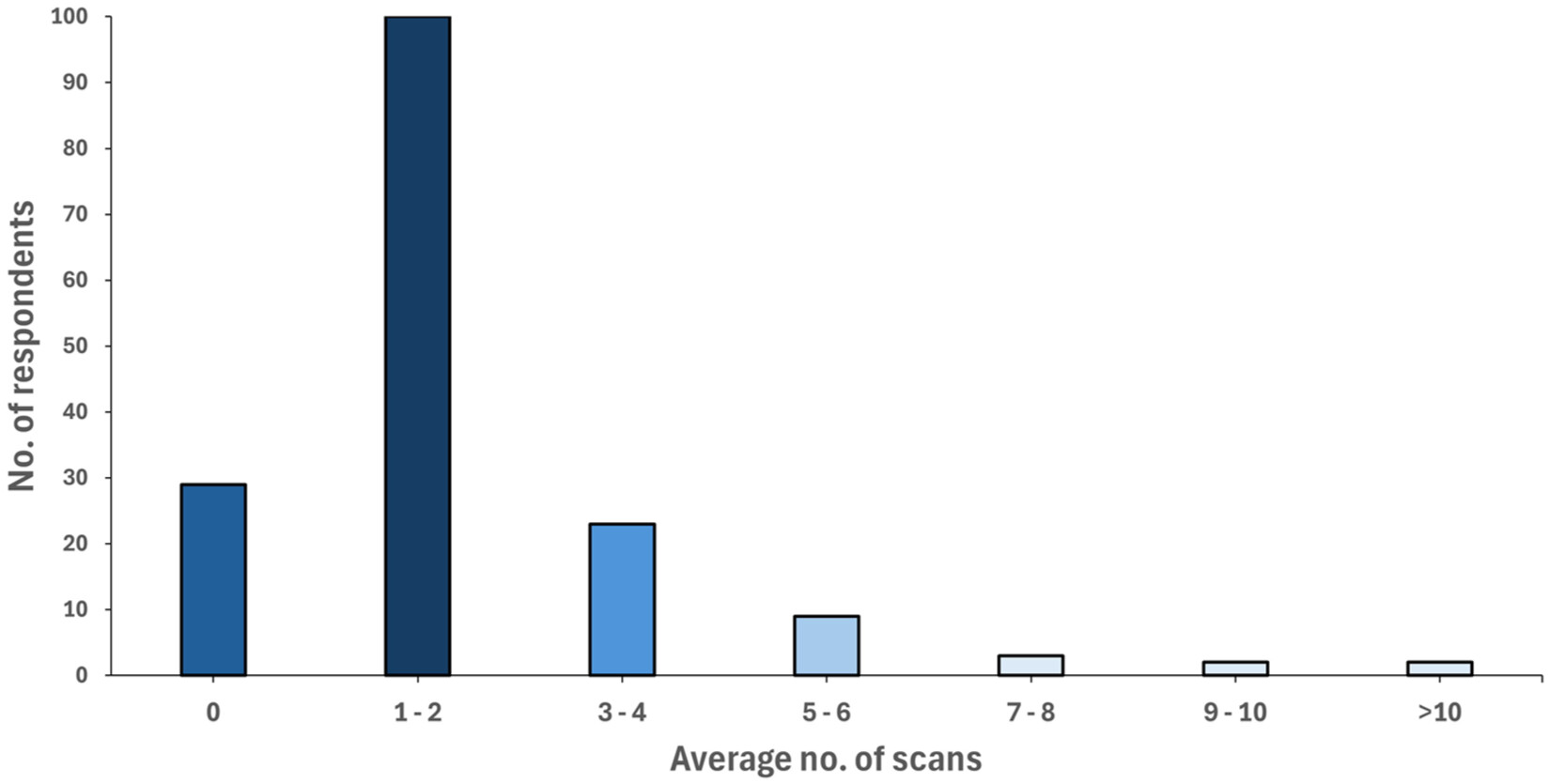
LUS utility in practice
| Respiration | Mechanical ventilation/liberation | ||
| Increased fraction of inspired oxygen (FiO2) | 80 | Difficult or slow to wean off ventilation | 31 |
| Low oxygen saturation (SpO2) | 24 | Unable to wean off ventilation | 20 |
| Unable to wean off oxygen | 6 | Increased ventilatory support | 17 |
| Respiratory failure | 6 | Reduced tidal volume | 6 |
| Difficult or slow to wean off oxygen | 4 | Difficult to ventilate | 4 |
| Hypercapnia | 1 | Patient and ventilator asynchrony | 1 |
| Respiratory acidosis | 1 | Reduced lung compliance | 1 |
| Failed extubation | 1 | ||
| Chest Radiograph (CXR) | Auscultation | ||
| Unclear CXR findings | 42 | Reduced breath sounds | 19 |
| CXR doesn’t correlate with patient presentation | 5 | Abnormal breath sounds | 11 |
| CXR absent/unavailable | 1 | Absent breath sounds | 1 |
| Diagnostic thinking | Therapeutic thinking | ||
| Check if pathology will respond to physiotherapy | 16 | To re-assess post-treatment | 14 |
| To aid clinical reasoning | 12 | To re-assess when treatment not effective | 7 |
| As part of the initial assessment on admission | 6 | To guide changes in treatment | 4 |
| To identify the presence of pathology | 3 | When patient isn’t meeting their expected milestones | 3 |
| Breathing | Other signs or symptoms | ||
| Increased work of breathing (WOB) | 6 | Increased sputum load | 15 |
| Increased respiratory rate (tachypnoea) | 2 | Dyspnoea | 1 |
| Reduced chest wall motion | 1 | Pain | 1 |
Educational resources during training and continuing professional development (CPD) post-accreditation
Discussion
Demographics
LUS accreditation training & mentoring
LUS implementation and governance
LUS utility in practice
Educational resources during training and continuing professional development (CPD) post-accreditation
Limitations
| Future areas for development |
| • Aim to meet existing ultrasound governance recommendations |
| • Develop a specific LUS guidance document for physiotherapists |
| • Boost training numbers with at least one mentor in every trust/health board |
| • Strengthen existing clinical areas and develop new areas of practice |
| • Develop communities of practice and shared CPD opportunities and resources |
| • Investigate how LUS can enhance the efficacy and efficiency of physiotherapy interventions |
| • Screening tool to better indicate which patients should receive a LUS. |
Conclusion
Acknowledgments
Ethical considerations
Consent for publication
Declaration of conflicting interests
Funding
ORCID iD
Data availability statement
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In

Keywords
Data availability statement
Authors
Author contributions
Metrics and citations
Metrics
Journals metrics
This article was published in Journal of the Intensive Care Society.
View All Journal MetricsPublication usage*
Total views and downloads: 686
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 0
Crossref:
There are no citing articles to show.
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Purchase 24 hour online access to view and download content.
Access journal content via a DeepDyve subscription or find out more about this option.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}