Introduction
Metformin is a widely prescribed medication for type 2 diabetes mellitus (T2DM) due to its efficacy in lowering blood glucose levels, enhancing insulin sensitivity, and minimizing cardiovascular risks.
1 The mechanism of action involves inhibiting hepatic gluconeogenesis, enhancing peripheral glucose uptake, and modulating gut microbiota.
2,3 Despite its favorable therapeutic profile, metformin’s safety has been debated due to its potential to elevate lactate levels, which, in rare cases, may progress to metformin-associated lactic acidosis (MALA).
4While MALA is rare, subclinical elevations in lactate levels may have clinical implications. Several studies have suggested that even mild elevations in lactate levels could contribute to metabolic distress, fatigue, and increased cardiovascular risk.
4,5 This risk is higher among vulnerable populations such as older patients, those with impaired renal function, and individuals with multiple comorbidities.
5,6Elevated lactate levels in metformin users can be attributed to impaired lactate clearance and increased anaerobic metabolism.
4 Metformin inhibits complex 1 of the mitochondrial respiratory chain, leading to a shift toward anaerobic glycolysis, thereby increasing lactate production.
7 In addition, the kidneys play a critical role in clearing metformin and lactate, and renal impairment is a key risk factor for lactate accumulation. Consequently, its use in patients with chronic renal disease or those receiving nephrotoxic drugs has raised safety concerns.
6Age-related physiological alterations additionally affect lactate levels in patients receiving metformin. Older adults experience age-related declines in renal function and mitochondrial efficacy, perhaps leading to an increased risk of lactate accumulation.
8,9 Previous studies have indicated a relationship between age and lactate levels, with older patients exhibiting elevated lactate levels attributed to reduced renal clearance; hence, dose adjustments in older populations may mitigate this risk.
6,10,11 In addition, polypharmacy, which is prevalent in older adults, increases the risk of drug–drug interactions and potentiates the effect of metformin on lactate metabolism. The concurrent prescription of non-steroidal anti-inflammatory drugs (NSAIDs) and diuretics may exacerbate lactate accumulation due to their impact on renal perfusion.
11,12Several studies have focused on MALA; however, there is little research examining the risk factors associated with subclinical lactate elevations. Understanding these characteristics is critical for enhancing metformin therapy, especially in vulnerable populations at risk of lactate accumulation. This study aims to determine the prevalence of elevated lactate levels in patients receiving metformin therapy attending outpatient endocrinology and internal medicine clinics, characterize the demographic and clinical characteristics of metformin users, and identify patient-specific risk factors associated with elevated lactate levels. This study’s findings improve our understanding of metformin’s safety profile and inform personalized prescribing strategies to optimize patient outcomes.
Methods
Study design, ethical considerations, and study population
This was a retrospective, cross-sectional study based on routinely collected medical records (secondary data analysis). Data for this study were collected as per the approval from the Institutional Review Board (IRB) at Mohammed Al-Mana College for Medical Sciences (SR/RP/79, Approval Date February 17, 2022) and the approval from the Qatif Central Hospital’s IRB (QCH-SRECO 19-2022, Approval Date June 8, 2022). Data were collected between the period of August 1, 2022 and February 20, 2023 from the hospital information technology department. All participants were deidentified and the waiver of consent collection was approved by IRB as data were collected retrospectively.
The inclusion criteria were patients aged 40 years or older who attended an outpatient endocrinology and internal medicine clinic and were diagnosed with T2DM between January 2020 and December 2021, with a completed medical record. The study cohort was limited to patients visiting outpatient endocrinology and internal medicine clinics to mitigate confounding associated with acute metabolic abnormalities. The set of 40 years as an inclusion criterion was selected, as older age is associated with a higher prevalence of multiple comorbidities, which could complicate T2DM management and influence lactate levels.
9,13Patients aged 40 years old and younger, attending surgical or other medical care clinics, or an emergency department, and not diagnosed with T2DM were excluded. Consequently, patients with acute critical illness, severe infection, sepsis, or hypoxic respiratory conditions throughout the duration of the study were not to be included. For patients with multiple visits during the study period, only data from their first reported visit were included.
This retrospective study utilized routinely collected clinical data; thus, a formal a priori sample size calculation was not conducted. Instead, all eligible patients who met the inclusion criteria during the study period were incorporated to enhance statistical power and precision of estimates.
Data collection, measures, and definitions
Demographic data, comorbidities, and recent laboratory findings were extracted from the medical electronic record, while the prescribed medications were verified from the pharmacy electronic records to ensure accurate representation of patient profiles. Comorbidities were identified and coded as per the International Classification of Diseases, 10th revision, 2016 (ICD-10).
14 Comorbidities identified in the literature to potentiate the risk of MALA were collected and documented as heart failure, anemia, thyroid diseases, liver diseases, and renal diseases.
11 The Charlson Comorbidities Index (CCI) was calculated to predict 1-year mortality risk, and the creatinine clearance (CrCl) was estimated using the Cockcroft-Gault Equation.
15,16 Significant laboratory tests linked to evaluate and assess elevated lactate level were identified as creatinine kinase (to determine level of muscle damage), random blood glucose and glycosylated hemoglobin (to evaluate level of T2DM management), hemoglobin (to assess level of anemia), lactate dehydrogenase, and lactate level (Table S1). Lactate concentration was analyzed as a continuous variable across all statistical models. In this study, the term “elevated lactate” represents a relative or marginal increase in comparison to the reference group, rather than values exceeding pathological thresholds.
Blood lactate levels were determined based on standard laboratory tests documented in the hospital’s electronic medical record system. Lactate testing was conducted as a component of routine outpatient clinical assessment or metabolic evaluation at the treating physician’s discretion, rather than following a study-mandated procedure. All measurements were derived from venous blood samples analyzed in the hospital’s central laboratory utilizing standardized automated enzymatic techniques.
Lactate levels for metformin users aligned with durations of active metformin therapy as recorded in pharmacy prescription data. The retrospective approach limited standardization of the precise timing relative to the most recent metformin dose; however, all patients included had active metformin prescriptions during lactate testing.
Serum creatinine levels used for calculating CrCl were obtained from laboratory tests performed during the same outpatient visit as the lactate measurement or within a maximum of 7 days. For patients with multiple creatinine measurements throughout this period, the value nearest to the lactate test date was used. Metformin exposure and daily dosage were confirmed as active during laboratory testing via pharmacy prescription records.
The medications data, including long-term regular, short-term, as-needed prescriptions, and supplements, were collected and coded as per the Anatomical Therapeutic Chemical (ATC) classification system.
17 From this list, the number of prescribed medications (NPM) was counted and documented. Furthermore, medications identified in the literature to potentiate the risk of MALA were documented as renin-angiotensin-aldosterone system inhibitors (RAASIs), diuretics, beta blockers (BBs), NSAIDs, antiepileptics, and systemic corticosteroid intake.
Records with missing values for the main outcome, blood lactate level, were excluded from the analysis. Analyses of other variables used only complete cases. The amount of missing data for the covariates was low, with less than 5% missing for each variable. Therefore, no imputation methods were applied.
Several potential sources of bias were considered. Selection bias was reduced by including all eligible patients who met the predefined criteria during the study period and by using electronic medical records instead of self-reported data. Information bias was reduced by extracting demographic, clinical, laboratory, and medication data in a standardized format from validated hospital electronic systems and pharmacy records. Misclassification bias was minimized by coding comorbidities with ICD-10 codes and medications using the ATC classification system.
In the current study, patients were classified based on their age into either middle-aged patients (<65 years) or older patients (⩾65 years) to assess the prevalence and pattern difference between these two groups in terms of metformin prescribing and prevalence of factors potentiating the risk of elevated lactate level. Furthermore, patients were classified based on the total daily metformin dose into low-dose users (⩽1000 mg/day), medium-dose users (1001–1500 mg/day), and high-dose users (⩾1501 mg/day) to assess the dose-dependent relationship with lactate level.
Statistical analysis
Demographic variables, comorbidities, and medication use were summarized using mean ± standard deviation (SD) for parametric continuous variables, median with interquartile range (IQR) for nonparametric continuous variables, and number with frequency (%) for categorical variables. For comparisons of continuous variables, the Student t test and the Mann–Whitney U test were used for parametric and nonparametric data, respectively. The Chi-square test was used to compare the frequency of categorical variables between groups. The pattern of metformin prescribing (difference in doses) and the difference between different metformin dosing groups were assessed using the analysis of variance test.
Multivariable linear regression was used to evaluate factors associated with higher lactate levels (continuous outcome) in metformin users. Variable selection was determined by (i) clinical plausibility and existing research on metformin-induced lactate elevation and (ii) statistical associations identified in univariable studies. The base adjustment set comprised age, sex, body weight, CrCl, CCI, and daily metformin dosage, as these variables were known or expected to influence lactate production/clearance and metformin exposure. All covariates were simultaneously incorporated into the final model (entry approach) to derive adjusted unstandardized regression coefficients (β) with 95% confidence intervals. Multicollinearity was evaluated by the variance inflation factor (VIF), where VIF values beyond 10 indicate concerning collinearity. To examine potential effect modification by age group, stratified multivariable analyses among older (⩾65 years) and middle-aged (<65 years) metformin users were conducted, using the same predetermined adjustment method.
Statistical analysis was performed using the SPSS statistical package version 26, whereas graphs were produced using GraphPad Prism software.
Reporting standards
The study’s findings were reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) standards, which are used for cross-sectional studies.
18Results
This study included a total of 3304 diabetic patients who met the inclusion criteria. Among the included patients, female and middle-aged individuals were dominant (53% and 56%, respectively;
Table 1). The median age of the entire cohort was 62 years (IQR 53–71), the average CCI score was 6 (SD ±2), the average CrCl was 94 mL/min (±42), the average body weight was 78 kg (±19), and the average NPM was 7 (±6) (
Table 1).
Table 1 presents that metformin users presented with a lower average CCI score (5 vs 6,
p < 0.001) compared to nonusers. In reference to the recent laboratory findings,
Table 1 shows that the average lactate level was 1.4 (±0.7), the average lactate dehydrogenase level was 212 (±83), and the average creatinine kinase level was 103 (±36). Metformin users exhibited a significantly higher average lactate level (1.9 vs 1,
p < 0.001), higher lactate dehydrogenase level (214 vs 207,
p = 0.02), and higher average glycosylated hemoglobin (7.2 vs 7.1,
p = 0.045) compared to nonusers (
Table 1).
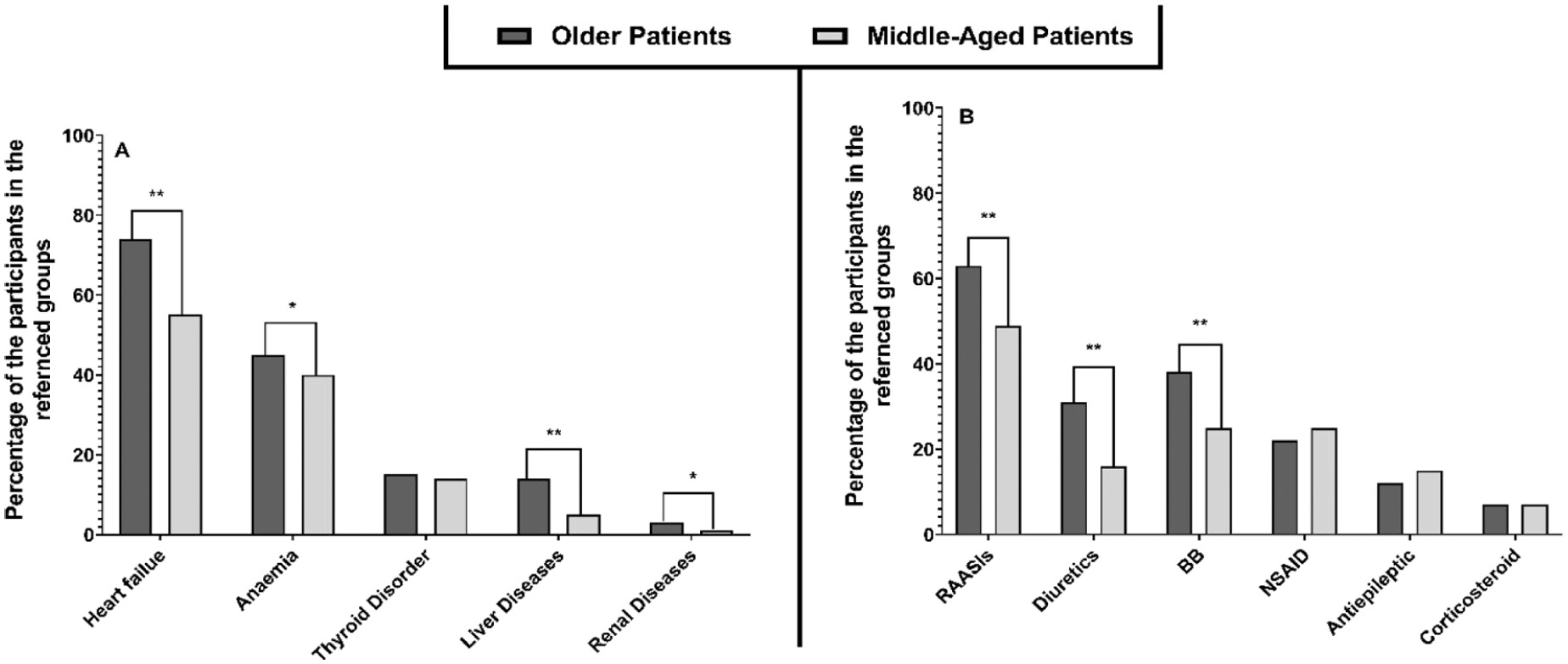
When investigating the prevalence of comorbidities that might potentiate the risk of elevated lactate level, the analysis revealed that heart failure (64% of the cohort), anemia (43%), liver disease (11%), and renal disease (7%) were the most prevalent morbidities (
Figure 1).
Figure 1 shows that metformin users were more likely to have thyroid disorders (15 vs 11,
p = 0.004) but less likely to have liver diseases (9 vs 15,
p < 0.001) and renal disease (2 vs 18,
p < 0.001) compared to nonusers.
Further analysis to determine the prevalence of coprescribing medications that may potentiate the risk of elevated lactate levels was performed, and the results revealed that RAASIs (52% of the cohort), BBs (34%), diuretics (26%), and NSAIDs (22%) were the most recorded medications (
Figure 1).
Figure 1 shows that metformin users were more often coprescribed RAASIs (55 vs 44,
p < 0.001) and NSAIDs (24 vs 18,
p < 0.001) but less likely to have diuretics (22 vs 36,
p < 0.001) and BBs (31 vs 42,
p < 0.001) compared to nonusers.
Among metformin users, 43% (
n = 991) were older adults, while 57% (
n = 1338) were middle-aged (
Table 2). Older patients were more likely to be female individuals (75% vs 63%,
p = 0.049), had higher average CCI scores (7 vs 4,
p < 0.001), lower average CrCl values (76 vs 107,
p < 0.001), and a lower average body weight (16 vs 19,
p < 0.001) compared to middle-aged patients (
Table 2). Interestingly,
Table 2 shows that older patients tend to have a higher average creatinine kinase blood level (106 vs 100,
p < 0.001) but a lower hemoglobin level (13.2 vs 13.6,
p = 0.02) compared to middle-aged users.
Further analysis to determine the difference between older versus middle-aged patients among metformin users was performed and the results revealed that older patients had a higher prevalence of heart failure (74% vs 55%,
p < 0.001), liver disease (14% vs 5%,
p < 0.001), anemia (45% vs 40%,
p = 0.01), and renal disease (3% vs 1%,
p = 0.01;
Figure 2).
Figure 2 shows that older patients had a higher rate of coprescribed medications, including RAASIs (63% vs 49%,
p < 0.001), diuretics (31% vs 16%,
p < 0.001), and BBs (38% vs 25%,
p < 0.001) compared to middle-aged patients.
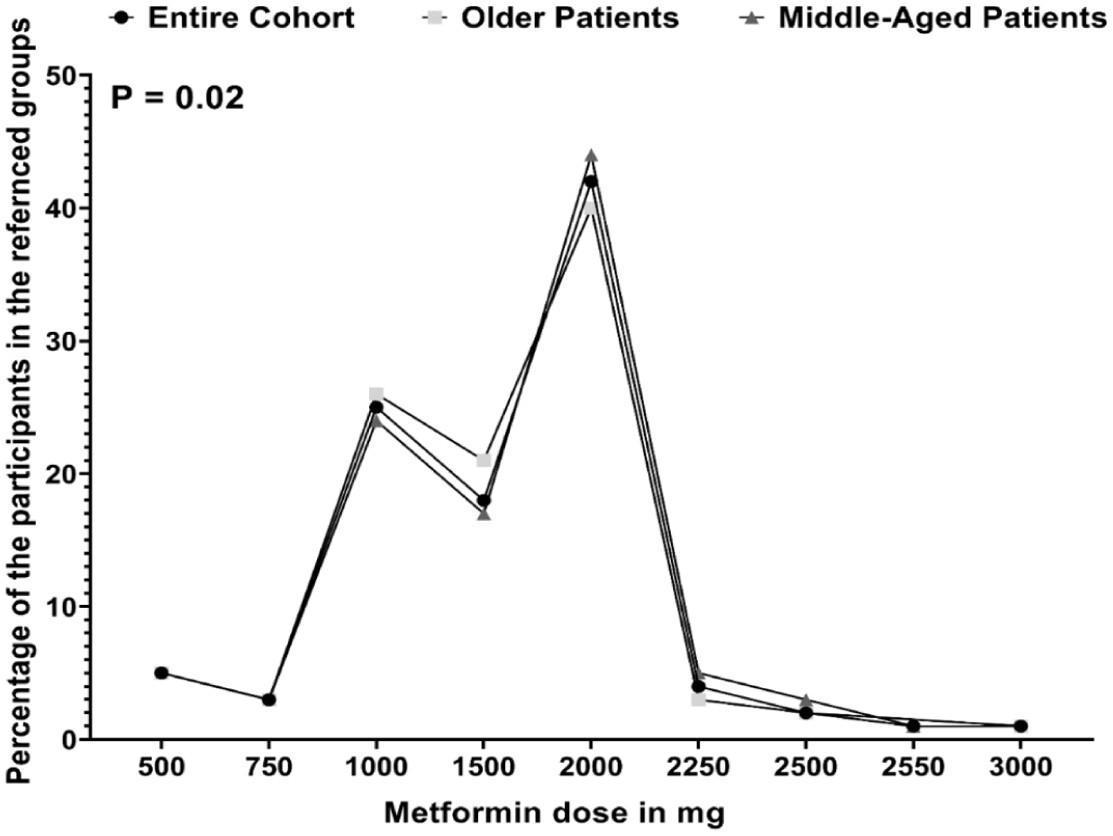
Further analysis was conducted to determine the pattern of metformin dosing among the entire cohort and to assess the pattern difference between older and middle-aged patients. The most commonly prescribed metformin dose was 2000 mg/day (42%), followed by 1000 mg/day (25%) and 1500 mg/day (18%;
Figure 3). Interestingly,
Figure 3 shows that older patients received more frequent doses of 1500 mg/day (21% vs 17%) and 1000 mg/day (26% vs 24%) but were less likely to receive a dose of 2000 mg/day (40% vs 44%,
p = 0.02) compared to middle-aged patients.
Further analysis revealed that medium-dose users were older compared to low-dose and high-dose users (64 vs 63 vs 62 years,
p < 0.001;
Table 3).
Table 3 presents that high-dose users were heavier (80 vs 79 vs 77 kg,
p = 0.012) and had a higher average CrCl (96 vs 92 vs 91,
p = 0.019) compared to medium-dose and low-dose users, respectively. Interestingly, the analysis concluded that high-dose users had a higher average lactate level (2.5 vs 2.4 vs 2.3,
p = 0.001) compared to medium-dose and low-dose users, respectively (
Table 3).
Figure 4 shows that high-dose users had a higher prevalence of heart failure (67% vs 64% vs 58%,
p = 0.001) and were prescribed RAASIs more often (59% vs 54% vs 48%,
p < 0.001) compared to medium-dose and low-dose users.
The multivariable regression analysis revealed that increasing metformin dose (β = 0.66,
p < 0.001) and age (β = 0.004,
p = 0.03) were associated with increasing lactate level among metformin users, whereas increasing CCI (β = −0.01,
p = 0.003) was negatively associated with elevated lactate level (
Table 4). In terms of comorbidities,
Table 4 presents that having renal diseases was associated with elevated lactate level (β = 0.2,
p < 0.001). Furthermore, the analysis revealed that coprescribing diuretics (β = 0.2,
p < 0.001), BB (β = 0.09,
p = 0.001), and NSAIDs (β = 0.1,
p = 0.001) were associated with elevated lactate level, whereas coprescribing RAASIs was negatively associated (β = −0.25,
p < 0.001;
Table 4). Further analysis to determine the factors associated with elevated lactate level among older users was conducted, and the results revealed that advancing age (β = 0.004,
p = 0.04), increasing metformin does (β = 0.68,
p < 0.001), having renal diseases (β = 0.2,
p < 0.001), and prescribing analeptics (β = 0.08,
p = 0.02) were associated with elevated lactate level (
Table 4). Interestingly, increasing the metformin doses (β = 0.65,
p < 0.001) and having renal diseases (β = 0.2,
p < 0.001) were associated with elevated lactate levels among middle-aged users (
Table 4).
Discussion
This study provides evidence to support that metformin use is associated with elevated lactate levels, with the degree of elevation being influenced by dosage, renal function, and concurrent medication use. These findings align with prior research indicating that metformin, while generally safe, can lead to subclinical lactate accumulation, especially in vulnerable populations.
4,11An important finding is that metformin users exhibited higher lactate levels in comparison to nonusers. Although this rise was statistically significant, the measured levels predominantly fell within the normal laboratory reference range, indicating borderline or high-normal elevations rather than clinically evident hyperlactatemia. This observation aligns with the established pharmacological effects of metformin, which suppress hepatic gluconeogenesis, enhance anaerobic metabolism, and result in elevated lactate production.
6 The reported lactate level is considered borderline and does inevitably advance to MALA. It is essential to recognize that even marginal elevations in lactate levels can be harmful, leading to metabolic stress, fatigue, and reduced exercise tolerance, particularly in patients with multiple comorbidities.
5,6 These findings indicate that proactive clinical monitoring is necessary to detect early signs and symptoms of elevated lactate levels, hence reducing potential complications associated with long-term metformin use.
The analysis of differences between metformin users and nonusers should be approached with caution. In this cohort, metformin users exhibited a lower prevalence of renal disease and a lower CCI compared to nonusers, reflecting clinical prescribing practices that avoid metformin for patients with significant renal impairment or complicated comorbidity profiles.
6,19 These baseline differences may independently affect lactate metabolism and thus partially explain the observed variations in lactate levels among groups. Accordingly, the comparison between metformin users and nonusers should be seen as descriptive rather than causal. To mitigate confounding, the principal inferential analyses focused exclusively on metformin users and utilized multivariable regression models that adjusted for significant variables. The adjusted findings provide a more rigorous evaluation of the factors associated with elevated lactate levels in the population exposed to metformin.
Another significant finding is the association between increasing metformin doses and elevated lactate levels. This dose-dependent relationship aligns with previous findings and advises careful monitoring for patients prescribed high metformin doses.
4,6 This study indicated that patients receiving high-doses of metformin exhibited improved renal function, indicating a prescribing pattern that favors higher metformin doses in patients with preserved clearance. However, this pattern does not exclude the risk of gradual lactate accumulation over time, particularly in older patients who typically have reduced CrCl and a higher CCI.
19 This phenomenon emphasizes the importance of individualized dose adjustments, particularly in older patients with a dose of >1500 mg/day of metformin.
Another important finding is the substantial association between coprescribing of diuretics and NSAIDs with elevated lactate levels. Diuretics induce dehydration and compromise renal perfusion, thereby hindering lactate clearance, while NSAIDs are recognized for reducing renal clearance, resulting in reduced renal perfusion and possible accumulation of metformin and lactate.
20,21 These findings emphasize the importance of pharmacist-led medication reviews in identifying drug–drug interactions and adverse drug reactions related to metformin prescribing, particularly in older patients. Interestingly, as NSAIDs are known to be over-the-counter medications, community pharmacists should take further precaution when dispensing NSAIDs for their patients, particularly for those who are older, diabetic, and using metformin.
In contrast, a key finding is that there is a negative association between the prescription of RAASIs and elevated lactate levels. A possible explanation for this association may be that RAASIs enhance renal perfusion and metabolic homeostasis, hence reducing lactate accumulation.
22,23 This finding must be interpreted cautiously and does not suggest a causal or protective effect, as the observational and cross-sectional design permits alternative explanations. Initially, confounding by indication might arise, as RAASIs are predominantly prescribed to patients with stable cardiovascular disease and preserved renal function, whereas those with advanced renal impairment or acute illness, who may be more susceptible to lactate elevation, are less likely to be administered these agents. Second, patients using RAASIs may demonstrate systematic disparities in disease severity, hydration status, and overall clinical stability relative to nonusers. Third, residual confounding from unmeasured variables such as dietary status, physical exercise, or medication adherence cannot be ruled out. Therefore, this finding suggests the need for further investigation to explore the potential protective role of RAASIs in minimizing the metabolic effects of metformin.
Another interesting finding is that the prevalence of comorbidities such as heart failure, anemia, and liver disease was higher among metformin users, but no significant associations were observed between these comorbidities and high lactate levels. Previous research had indicated that these conditions may impair lactate clearance, further increasing the risk of high lactate levels.
24 Interestingly, this study revealed that older patients were more likely to have these comorbidities, which could exacerbate lactate elevation. Given the fact that the prevalence of polypharmacy is higher among older patients, this could potentiate the risk of lactate level elevation.
25 These findings suggest a tailored metformin therapy to ensure balance between efficacy and safety among older patients.
10,25Another key finding is the association between renal diseases and elevated lactate levels. Metformin is renally cleared; thus, reduced renal clearance may result in metformin accumulation, potentiating its effects on lactate metabolism.
19 Interestingly, the current study could not establish a significant association between CrCl and lactate level, but it is worth noting that older patients presented with lower CrCl, which further potentiates their risk of borderline elevated lactate level, in addition to the previous factors discussed.
The current study supports earlier findings that metformin is generally well-tolerated; however, it necessitates vigilant monitoring in specific populations.
1,19,26 Our findings collectively advocate for routine lactate levels monitoring, especially in high-risk populations, including older adults, patients with renal impairment, and patients on high-dose metformin therapy. Although MALA remains rare, borderline elevated lactate levels should not be disregarded, as they may contribute to patient morbidity over time.
5 In addition, the current study emphasizes the value of individualized prescribing practices, particularly for older patients. Current guidelines recommend initiating metformin at a low-dose which can be titrated gradually while monitoring renal function and potential drug–drug interactions.
27,28 Prescribers and pharmacists should exercise increased vigilance when prescribing metformin in the presence of coprescribed diuretics, NSAIDs, or BBs. Given the increasing prevalence of T2DM among older patients, strategies (e.g., reducing metformin doses in patients with declining renal function or switching to alternative glucose-lowering agents) should be considered to optimize patient outcomes.
29 Longitudinal studies are needed, as future directions, to assess whether chronic exposure to high lactate levels leads to adverse metabolic outcomes. Future research should incorporate dietary and lifestyle factors to provide a more comprehensive understanding of lactate dynamics in metformin users.
This study has several strengths that should be acknowledged. This study represents the first investigation of elevated lactate levels associated with metformin use in an outpatient population, whereas prior studies focused on lactate levels in critically ill patients on metformin or the risk of MALA.
5,6 A large sample size enhances the external validity and supports the generalizability of our findings to the Saudi Arabian population. The comprehensive analysis, by classifying patients according to age and metformin dosage and incorporating multivariable linear regression, offers robust statistical power and facilitates a more detailed assessment of factors influencing lactate levels in metformin users.
Limitations
While this study has several strengths; yet, it is important to acknowledge specific limitations. First, the cross-sectional design restricts the ability to establish causality between metformin use and lactate elevation. However, regression models were applied to identify associated factors to overcome this limitation. This study is based on data collected from a single center, which may limit the generalizability to broader populations with different demographic and clinical characteristics. However, the large sample size with the diverse characteristics supports generalizability to the Saudi Arabian and Middle Eastern populations. Because the study was conducted in an outpatient setting, which diminishes the probability of severe acute illness, important clinical data regarding transitory illnesses, inflammatory states, or subclinical hypoxic conditions were often inaccessible and therefore could not be incorporated into the regression models. Residual confounding from acute physiological stressors cannot be entirely ruled out and may have affected lactate levels in a limited subset of patients.
29 Lactate levels were assessed at a single time point, limiting the ability to evaluate longitudinal changes or fluctuations in lactate metabolism. Additionally, lactate measurements were obtained during routine clinical care rather than at standardized time points relative to medication dosing, which may introduce variability in observed concentrations. Although CrCl and lactate levels were being measured during the same clinical period, the retrospective design of the study limited accurate synchronization with the precise timing of metformin administration. Consequently, transient variations in renal function or lactate associated with recent administration could not be entirely documented.
Lastly, as a cross-sectional study, lactate measurements were obtained during routine outpatient visits and were not associated with documented acute clinical symptoms, hospitalizations, or hemodynamic instability at the time of testing. Therefore, no direct short-term clinical effects attributable to lactate elevation were detected in our cohort.