Introduction
Child marriage is defined as a formal marriage or informal union below 18 years old. It can cause lifetime disadvantage and deprivation for minors especially females; however, it is still widespread in developing countries. It has been reported by the
United Nations Children’s Fund (UNICEF, 2018) that child marriage would severely compromise the well-being of the married adolescent girls when they go through such experiences as early pregnancy, social isolation, unable to continue schooling, limited opportunities for career and vocational advancement, and increased risk of domestic violence.
World Health Organization (WHO, 2013) reported that more than 140 million girls globally will become child brides between 2011 and 2020. There is a growing research interest concerning the driving forces of child marriage, and its implication for the health of female adolescents underscores the need for valid measures to assess the female adolescents’ attitudes toward child marriage.
The social and cultural contexts behind child marriage are not evident but wide-ranging, including prevailing gender inequality. In Bangladesh, it is reported that female sexuality is controlled through early marriage (
Chowdhury, 2004). Also, one of the main reasons for child marriage is family poverty. Parents in some of the developing countries believe that the girls are an economic burden to the family and decide to marry off their daughters early (
Parsons et al., 2015;
Petroni et al., 2017). This further leads to a lack of opportunity for the girls to receive education and an inability to participate in the labor force. Globally, there are some known health consequences of child marriage such as problems associated with early intercourse and pregnancy including infant and maternal mortality, repeated pregnancies, the risk for HIV, and other sexually transmitted diseases as well as depression (
Ferdousi, 2014;
Mahato, 2016;
Nour, 2006;
Svanemyr et al., 2015). There are other social and economic consequences such as a denial of childhood, social isolation, the restriction of personal freedom, and the lack of educational opportunity (
Ferdousi, 2014;
Mahato, 2016). It is also notable that child marriage persists through generation by generation; thus, the daughters will likely be facing the same cycle of childhood deprivation as their mothers experienced, who was also married at a young age. There are some programs and policies to prevent child marriage which had shown some evidence for improvement. According to
Lee-Rife et al. (2012), the programs that offered incentives and empowered the girls with the information, skills, and support networks in the developing countries had worked to prevent child marriage. Also, enhancing the accessibility for schooling allow girls to be engaged in staying at school and not to quit school due to child marriage (
Brown, 2012). Furthermore, by educating and mobilizing the parents, we can anticipate the changes in the social norms of the parents concerning the age of marriage of their daughters (
Nour, 2006). Currently, there is no scale to assess the attitudes, perceptions, or opinions about child marriage. The reason for the absence of such a scale may be due to the current main approach of retrospective examination of background after the cases of child marriage become a critical problem in society. If a prospective approach to foresee female adolescents’ attitudes toward child marriage is taken, it can be reflected as the views of the target groups to develop prevention programs for child marriage. The typical programs and activities to prevent child marriage are closely linked with measures to overcome the already-existing problems such as poverty and school dropouts. However, there seems no program that foresees potential tendencies among female adolescents toward child marriage such as personality and perception about premarital sex. Malaysia, an emerging economy in Southeast Asia, is one of such countries facing the problem of child marriage.
There is a scarcity of reliable statistics to report the official rate of child marriage in Malaysia. According to the latest census in 2010, the ratio of adolescent girls who are married between 15 and 19 years old in Malaysia is about 6% within population of that age range (
Kohno et al., 2019). The country is in its growth transition phase of an emerging economy and aiming to obtain developed nation status by 2030. The literacy rate of the youth aged 15 to 24 years in Malaysia is quite high with 97% as of 2018 (
UNESCO Institute of Statistics, 2020). The use of digital devices such as mobile phones is increasing among the youths in Malaysia. However, there is a digital divide between rural and urban youths (
Mohamed et al., 2012). Concerning religious norms and sexuality among Malay youths in Malaysia, the previous study reported that religious activities reduced the risk of continuing sexual activity for female youths but not for male youths. (
Muhammad et al., 2017). Under the current legal framework as of December 2018, it is not illegal for female adolescents below 18 years old to be married in Malaysia. Among many reasons why child marriage is socially allowed, one is the Muslim religious value that permits girls to be married after the onset of puberty, coupled with the perception that pregnancy out of wedlock is a sin (
Kohno et al., 2019,
2020;
Sudan, 2015;
Sudan et al., 2012). When parents know that their unmarried daughter is pregnant, they marry off the daughter quickly to avoid the sins of having a baby out of wedlock by the Muslim religious belief and to preserve the family’s dignity. However, a recent statement of concern was raised by a member of Parliament to not blame religion as a reason for child marriage but to focus on the health, psychological, and social implications of the girls who go through child marriage (
Ho, 2017). Also, the traditional value and culture supporting child marriage remain common among the ethnic minorities on Borneo Island (
Hin, 2017;
Kohno et al., 2020). In this context, there is a growing concern against child marriage in Malaysia, which catches media attention as well as concerns of the general public. Also, teenage pregnancy is on the rise in Malaysia, which is a flip of the same coin as child marriage, as most of the teenage pregnant girls out of wedlock either chose to or unable to get married when they find out about pregnancy outside of wedlock (
Mohd et al., 2015; K.
Omar et al., 2010). Considering this, it can be argued that a measurement scale that allows assessing female adolescents’ attitudes toward child marriage in Malaysia would make a unique contribution to understand why some of the girls get married underage in Malaysia. There is an existing scale that focused on measuring the attitudes of university students toward their parents and about marriage in Northern Cyprus (
Görkem & Bengisoy, 2018). Another study, although not in the form of the scale, investigated the effects of female youth’s attitudes on teenage premarital pregnancy in the United States and revealed the factors associated with premarital pregnancy are self-esteem, attitudes toward school, attitudes toward women’s family roles, and educational expectations (
Plotnick, 1992).
Valid and reliable measures of attitudes toward child marriage would allow for comparison of responses among female adolescents of different cultural and socioeconomic backgrounds and would allow policy makers and health practitioners to identify what constitutes the attitudes toward child marriage. Therefore, the aim of this study was to develop a multi-dimensional, self-administered scale to measure the attitudes toward child marriage among female adolescents in Malaysia.
Results
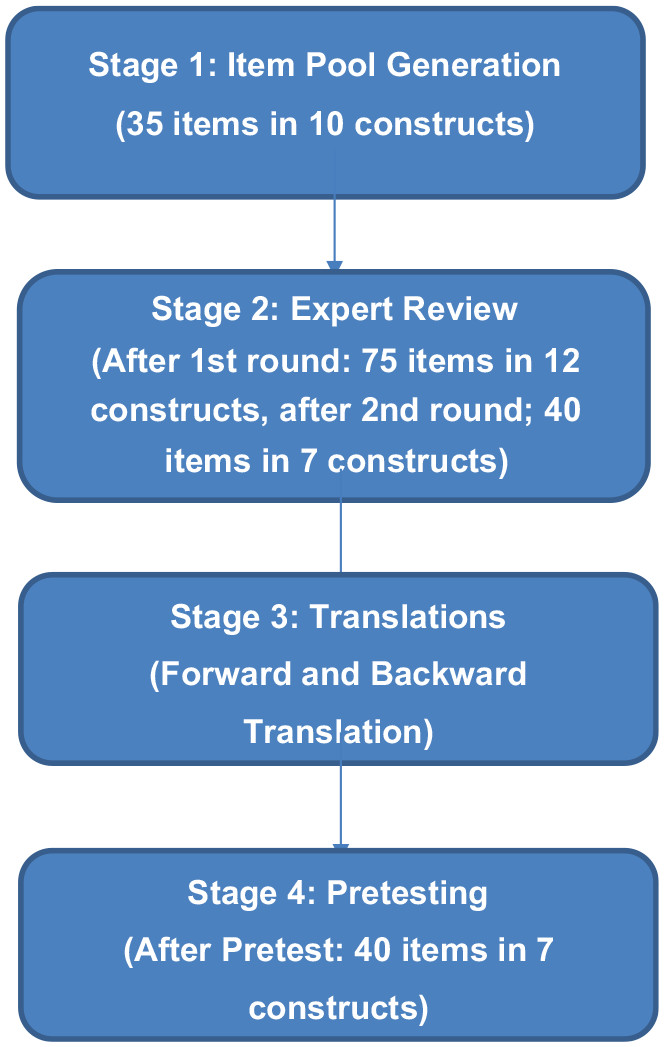
The EMAS is a 40-item questionnaire with Likert-type response purporting to measure the female adolescents’ attitudes toward child marriage. The instrument is designed to elucidate the following seven domains: (a) intuitive decision making, (b) believing in fate, (c) parental economic hardship during adolescence, (d) spiritual belief, (e) social norms, (f) opinion about premarital sex, and (g) relationship with parents/guardians. The initial draft of EMAS before expert review consisted of 10 domains, which was reduced after refinement. The initial construct of “religiosity” was modified as “spiritual belief” with the definition of “a religious conviction relating to the human spirit or soul as opposed to material or physical things.” Also, a new construct of “relationship with parents/guardians” was added, with the definition of “the state of being connected to a father, a mother and/or guardians.”
Expert Review
The CVI was calculated using data of experts’ evaluation of fit to objective (
Table 2), and I-CVI is available in
Online Appendix B. As the CVI for all constructs were above the prespecified value, all constructs were maintained and proceed to the next step. The experts were also invited to create new items if they felt that the provided list of item pools did not sufficiently reflect what it purports to assess in each construct. This procedure was added as a way to improve the content validity of the developed scale by obtaining a proper representation of the constructs (
Hardesty & Bearden, 2004).
The experts suggested 40 new items (available in
Online Appendix C), which led to the second version of the item pool of 12 constructs with 75 items. Among the added items, two of them were adapted from the Duke University Religion Index (DUREL), a scale on religiosity (
Koenig Harold et al., 1997). The three researchers (A.K., M.D., and N.D.N.F.) selected the items by carefully reviewing the expanded item pool, with the mind of a parsimonious selection of items to only select the items which are deemed pertinent. In the end, seven constructs with 44 questions were chosen as the finalized item pool. The list of revised item pool at the second round of expert review is shown in
Online Appendix D. This time, five experts were asked to evaluate the relevance of each item against the construct definition, by choosing their responses from four options (not relevant, somewhat relevant, relevant, very relevant). The expert agreement meant that the scores of either 3 (relevant) or 4 (very relevant) were chosen. CVI scores for each item were calculated, and the cutoff score of 0.78 was prespecified.
Table 3 shows the CVI for each construct concerning the evaluation of relevance in the second round of expert review, before and after item deletion. I-CVI values for each item in the second round of expert review are shown in
Online Appendix E.
In the second round of expert review, four items with low I-CVI values from the item pool were eliminated and resulted in seven constructs with 40 items. The values of mean CVI for each construct were above the prespecified cutoff point even before the elimination of four items but improved after item reduction (
Table 4).
Table 4 shows the list of finalized items before translations and pretesting.
Pretesting
Thirty female adolescents participated in the pretest that took place in October 2018. The mean age was 15.8 years; the majority are attending secondary school, are Malay ethnicity (73%), embrace Islam (77%), and are current students (83%). The socio-demographic information of the respondents is shown in
Table 5.
It took 10 to 25 min for them to complete the questionnaire, and on average, it took 5 min for the debriefing interview. Due to the illiteracy of one respondent, the scale was administered to her as an interview mode, by the interviewer reading the questions aloud, and based on the oral responses from this respondent, the interviewer marked down the responses in the response sheet on her behalf. It took 1 hr to complete the scale in this way.
The summary data of the score are shown in
Table 6 (details are available in
Online Appendix F). The percentage of midpoint responses out of all possible responses was 15% (179/1,200). The percentage of “I don’t understand” responses out of all possible responses was 0.75% (9/1,200). The percentage of missing data (no response) was 0.33% (4/1,200).
Data Analysis
The data were analyzed descriptively.
Table 7 shows the construct evaluation measures.
As shown in
Table 7, most of the mean scores for each construct are fair. The low means were observed for the construct of “Opinion About Premarital Sex,” which indicates that the respondents tend to have a conservative view toward this construct. There was no outlier in these data by checking the box plots of the scores for each construct. There were some missing values, and the mean imputation method was used. Missing data were substituted with the mean value of that item. Therefore, it can be concluded that the items in this scale were understood properly by the respondents in this pretest, and the scale is relevant to this group in demonstrating a common ground.
The analysis of the debriefing data was conducted by assigning codes and counting frequencies. The transcripts of the debriefing were analyzed by checking the response to the four questions. The summary of codes is described in
Table 8.
Based on the results of the analysis of debriefing data concerning Scale Contents, the content of the scale was understood by about half of the respondents. In terms of unclear wording, some specific words were difficult for some of the respondents to understand. For example, some of them did not understand what it means by “follow the instinct.” They know the word “instinct,” but it is not clear for them to conceptually imagine what the situation is like, because of lack of life experience. In terms of the scale length, most of the respondents stated that it is adequate. Concerning the addition of questions, although there were some minor opinions to add questions on a relationship with friends and individual emotions, it was decided not to include them in the scale, to maintain the scope of this scale.
The open-ended discussions were conducted between the respondents and the interviewer, concerning what was the impression the respondents had about the topic of child marriage. Some of the respondents understood that child marriage is a bad thing, and by taking part in the research, they can help prevent child marriage. Some of them clearly stated that pregnancy is the reason why some of the girls get married at a young age. They also raised concerns that those girls who get married at a young age do not know what the risks of child marriage are. The girls knew that those who get marry early are not afraid of the potential risks associated with child marriage because they are unaware of such risks. Other respondents thought it is normal to get married at a young age, as they see their friends and acquaintances getting married early.
Discussion
In this study, a scale to measure the attitudes toward child marriage (EMAS) was developed and pretested among female adolescents, aged between 15 and 17 years old, in Malaysia. It is well known that this age range is the time when some of the girls who are vulnerable to the risk of child marriage would encounter the possibility of choosing child marriage, due to such factors as an experience of premarital sex or pregnancy. Therefore, it is important to assess the attitudes of young female adolescents toward child marriage, before they are exposed to such risks critically. Various studies on adolescent health take into consideration of the appropriate age of the target group. For example, in the study of adolescent pregnancy outcomes and risk factors in Malaysia, the girls aged 10 through 19 years were targeted for analysis (K.
Omar et al., 2010). In the study asking about premarital sexual intercourse, the study targeted students aged 12 through 19 years old (
Lee et al., 2006). The study of the determinants of sexual intercourse among unmarried youths in Malaysia targeted unmarried girls aged between 15 and 21 years old (
Zulkifli & Low, 2000). Some of the studies include as young as 10 years old. However, in our study, it is not necessary to include those youngest adolescent group aged 10 to 14 years old, as the subject matter included in this scale may be sensitive and something they have never thought about before. Although a recent case of child marriage of an 11-year-old girl marrying a 41-year-old man shocked Malaysian society, and it can be observed that lowering the age of marriage in extreme cases is perceived as a problem in Malaysia, it is still a rare case (“
41-Year-Old Man Wanted to Marry Child Bride Since She Was 7,” 2018). Considering the age range of the target group in the aforementioned studies, and the discussion points as elaborated earlier, it is recommended that the targeted age range for this scale should be set conservatively as the female adolescents aged between 15 and 17 years old.
Another aspect of the discussion is the scoring method, including the format of the response options for this scale. In this scale, it is recommended to adopt the 4-point Likert-type scale response options without the midpoint response: strongly agree, agree, disagree, strongly disagree. This is because of the response observed from the pretest, as well as two arguments made by the studies concerning scale development by other researchers. One argument is that, in the longitudinal study of asking about political opinion, the young adolescent group (12–14 years old) tended to choose relatively more midpoint options, compared with the older adolescent group (18 years old and above) (
Raaijmakers et al., 2000). Another researcher pointed out that, given the limitations of children’s cognitive ability and communicative and social skills, it is expected that they are sensitive to “the temptation to satisfice by choosing a neutral mid-point when this is not the optimal answer” (
Borgers et al., 2004, p. 20). Furthermore, in our study, the rate of choosing the midpoint response was 15% out of all possible responses. This rate is not outstanding, yet may be improved if the response with a clear direction was chosen. Considering these findings, therefore, it is recommended that this scale adopts the response options without midpoint. Taking into consideration, the scoring method shall be determined as a future study, once further validity and reliability tests have been completed.
Regarding the comprehensiveness of the instrument, the debriefing analysis revealed the scale was well received by the assumed target group. Only a few participants reported some difficulty understanding the words used in the questions. Therefore, it is recommended that this scale be administered as self-administration mode, with the option of reading aloud to the respondents who have reading difficulty. In a future study, it is recommended to add explanations to those words which were deemed difficult, to enhance understanding, but not to change the words of the items of this scale, as it is important to maintain these words, and given that the response was relatively few.
The implication of this study to the health of adolescents is numerous. One obvious advantage is to be able to assess their perceptions about child marriage as scores, which can be utilized to come up with the policies and programs regarding adolescent health. The scale consists of such construct as an opinion about premarital sex. By understanding the adolescent girls’ perception of premarital sex, the data can be used to develop educational materials that support and empower adolescent girls with more adequate knowledge of sexual health. Another implication is that this scale can be used for health promotion. The summary scores of EMAS can be used to communicate and heighten the awareness of not only the girls but also the parents, teachers, and other community members who play an important role in the improvement process of adolescent health.
Strengths and Limitations
This is the first scale developed to assess the attitudes of female adolescents toward child marriage. The development process was comprehensive as a qualitative study, literature review, expert review, and the feedback obtained from the targeted group in the debriefing interviews during the pretest. Because it is important to hear from the adolescent girls about their perceptions and attitudes toward child marriage, by doing so, we can enhance understanding of what are the variables that are influencing their decisions concerning child marriage, and reflect the voices of the girls who may be exposed to the risk of child marriage in a tangible form as the scale scores. We believe that this scale can be utilized by the practitioners and government officers who oversee in creating policies to prevent child marriage, to capture the real perception and attitudes of the adolescent girls related to the 10 constructs that are included in this scale. Limitations of this study are that this scale as its current form includes redundancy of the items, which is purposefully maintained at this stage. The elimination of redundancy shall be based on the results of factor analysis with several hundred participants. Also, bias arising from the question order and other sources were not explored in this study. Furthermore, an open-ended question may add values by collecting data that reflect the true feelings of the respondents. Therefore, such a question as “Why do you think some girls get married before the age of 18?” can be added to this EMAS scale. The scores of EMAS during the pretest must be interpreted with caution as some respondents chose the response option of “I don’t understand the question.” In such a case, they received zero points; therefore, the score may not represent the results fairly. Hence, this pretest resulted in just tentative conclusions about the contents. Another limitation is concerning the applicability of this scale to multiple ethnic groups. Most of the respondents in the pretest were Malay ethnic group, with some Indians, but there were no representatives from Chinese. Therefore, caution is required when adopting this scale to all ethnicities even in Malaysia. The EMAS as in its current form must be checked for reliability and validity by applying this to a larger sample as a pilot test and conduct factor analysis for the considerations of item reduction and identification and confirmation of distinct constructs before usage. In future studies, the authors aim to identify and delete the redundant items, the least useful, and irrelevant, to produce a concise instrument with a minimum number of items and allow for wider usage in various settings. Furthermore, EMAS can be used in cross-cultural research as items are made available in English, although the items must go through the pretest for content validation. In the end, the EMAS is a good measure of assessing female adolescents’ attitudes toward child marriage and can be applied once the necessary validations are conducted.