

Married Women Decision-Making Autonomy on Contraceptive Use in East Africa: A Multilevel Analysis of Recent Demographic and Health Survey
Abstract
Background
Methods
| Regions | Countries | Year of survey | Weighted sample (n) | Percentage (%) |
|---|---|---|---|---|
| Burundi | 2016/17 | 2,792 | 6.66 | |
| Comoros | 2012 | 632 | 1.51 | |
| Ethiopia | 2016 | 3,669 | 8.76 | |
| Kenya | 2014 | 5,035 | 12.02 | |
| Malawi | 2015/16 | 9,552 | 22.80 | |
| Mozambique | 2011 | 1,086 | 2.59 | |
| Rwanda | 2014/15 | 3,706 | 8.85 | |
| Tanzania | 2015/16 | 3,149 | 7.52 | |
| Uganda | 2016 | 4,373 | 10.44 | |
| Zambia | 2018 | 3,794 | 9.06 | |
| Zimbabwe | 2015 | 4,107 | 9.80 | |
| Total sample size | 41,893 | 100 |
Variables of the Study

| Variables | Description |
|---|---|
| Individual level variables | |
| Age of the women’s | 15–24, 25–34, and 35+ |
| Resident | Rural, Urban |
| Women education Level | No formal education, Primary education, and Secondary education and higher |
| Women occupation | Not employed, employed |
| Partner education level | No formal education, Primary education, and Secondary education and higher |
| Wealth index | It was categorized as Poor, Middle and Rich |
| Number of living children | ≤2, >2 |
| Visited health facility last 12 months | No, Yes |
| Media exposure to family planning message | No, Yes |
| Community level variables | |
| Perceived distance to the health facilities | Big problem, Not big problem |
| Community level education | High, Low |
| Income level | Low income, lower middle income |
| Community level media exposure to family planning message | High, Low |
| Country | Burundi, Comoros, Ethiopia, Kenya, Malawi, Mozambique, Rwanda, Tanzania, Uganda, Zambia and Zimbabwe |
Data Analysis
Results
Individual and Community Level Factors
| Variables | Category | Frequency | Percent |
|---|---|---|---|
| Age in years | 15–24 | 9,003 | 21.49 |
| 25–34 | 18,531 | 44.23 | |
| ≥35 | 14,360 | 34.28 | |
| Educational status of women | No formal | 6,497 | 15.51 |
| Primary | 22,452 | 53.59 | |
| Secondary & Higher | 12,945 | 30.90 | |
| Husband education | No formal | 5,350 | 12.78 |
| Primary | 20,139 | 48.09 | |
| Secondary and higher | 16,389 | 39.14 | |
| Occupation of respondents | Not employed | 10,930 | 26.12 |
| Employed | 30,918 | 73.88 | |
| Wealth index | Poor | 13,381 | 32.89 |
| Middle | 8,301 | 19.81 | |
| Rich | 19,812 | 47.29 | |
| Media exposure to family planning message | Yes | 3,549 | 51.12 |
| No | 3,394 | 48.88 | |
| Number of living children | ≤2 | 16,317 | 38.95 |
| >2 | 25,577 | 61.05 | |
| Visited the health facility in the last 12 months | Yes | 30,120 | 71.90 |
| No | 11,771 | 28.10 | |
| Intimate partner violence | Yes No | 3,242 4,659 | 41.03 58.97 |
| Distance to the health facility | Big problem | 15,833 | 37.80 |
| Not big problem | 26,060 | 62.20 | |
| Residence | Urban | 12,150 | 29.00 |
| Rural | 29,743 | 71.00 | |
| Community media exposure to family planning | High | 17,899 | 50.10 |
| Low | 17,827 | 49.90 | |
| Community level education | High | 19,689 | 47.00 |
| Low | 22,204 | 53.00 | |
| Income level | Low income | 33,064 | 78.92 |
| Lower middle | 8,829 | 21.08 |
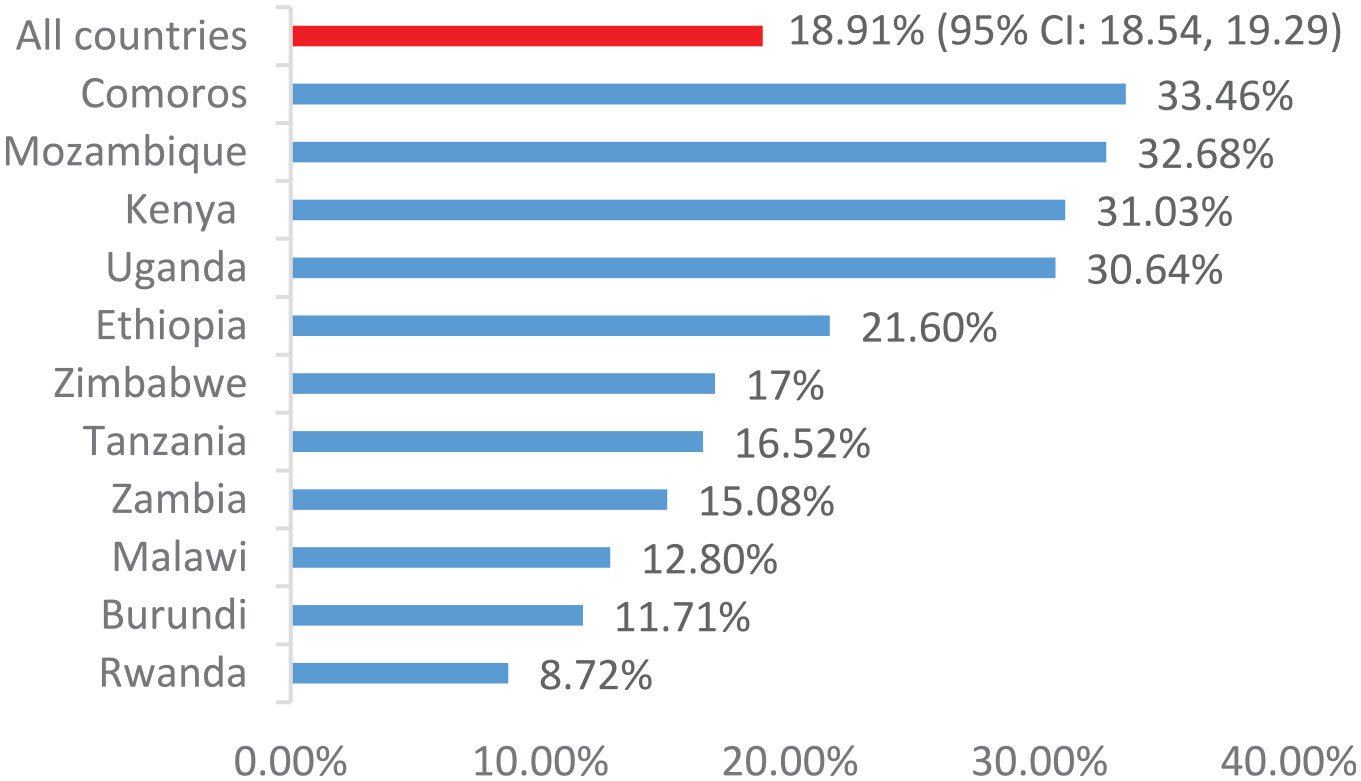
Women’s Decision-Making Autonomy on Contraceptive Use in East Africa
Factors Associated With Women Decision-Making Autonomy on Contraceptive Use
| Variables | Categories | Null model | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|---|
| AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | |||
| Age | 15–24 | 1 | 1 | ||
| 25–34 | 0.95(0.76, 1.20) | 0.95(0.75, 1.17) | |||
| ≥35 | 1.08(0.83, 1.39) | 1.07(0.82, 1.37) | |||
| Women education status | No formal education | 1 | 1 | ||
| Primary | 0.87(0.69, 1.09) | 0.90(0.70, 1.06) | |||
| Secondary and Higher | 0.75(0.57, 0.99) | 0.76(0.59, 1.03) | |||
| Husband education status | No formal education | 1 | 1 | ||
| Primary | 0.92(0.72, 1.19) | 0.93(0.72, 1.20) | |||
| Secondary and Higher | 0.79(0.60, 1.05) | 0.78(0.58, 1.03) | |||
| Occupation of women | Non-employed | 1 | 1 | ||
| Employed | 1.20(1.01, 1.42) | 1.24(1.03, 1.44)* | |||
| Wealth index | Poor | 1 | 1 | ||
| Middle | 0.81(0.65, 0.98) | 0.77(0.64, 1.04) | |||
| Rich | 1.04(0.85, 1.26) | 0.86(0.69, 1.12) | |||
| Media exposure to family planning message | No | 1 | 1 | ||
| Yes | 1.02(0.88, 1.18) | 1.07(0.92, 1.24) | |||
| Number of living children | ≤2 | 1 | 1 | ||
| >2 | 1.35(1.11, 1.64) | 1.38(1.13, 1.67)* | |||
| Visited the health facility in the last 12 months | No | 1 | 1 | ||
| Yes | 1.22(1.04, 1.44) | 1.22(1.05, 1.45)* | |||
| Perceived distance to health facility | Big problem | 1 | 1 | ||
| Not big problem | 1.05(0.98, 1.11) | 1.04(0.89, 1.19) | |||
| Residence | Rural | 1 | 1 | ||
| Urban | 1.42(1.31, 1.47) | 1.39(1.27, 1.50)* | |||
| Community media exposure to family planning message | Low | 1 | 1 | ||
| High | 1.03(0.94, 1.11) | 1.25(1.04, 1.45)* | |||
| Community level education | Low | 1 | 1 | ||
| High | 0.91(0.83, 0.97) | 0.97(0.81, 1.17) | |||
| Country | Rwanda | 1 | 1 | ||
| Burundi | 1.40 (1.19, 1.66) | 1.34(1.13, 1.58) | |||
| Comoros | 5.09 (4.13, 6.27) | 5.29 (4.26, 6.58) | |||
| Ethiopia | 2.95 (2.55, 3.42) | 2.94 (2.52, 3.44) | |||
| Kenya | 5.66 (4.88, 6.57) | 6.40 (5.51, 7.44) | |||
| Malawi | 1.62 (1.41, 1.87) | 1.8 (1.56, 2.08) | |||
| Mozambique | 5.03 (4.21, 6.01) | 5.61 (4.68, 6.74) | |||
| Tanzania | 1.42 (0.96, 2.08) | 1.42 (0.93, 1.97 | |||
| Uganda | 4.85 (4.24, 5.55) | 5.41 (4.70, 6.21) | |||
| Zambia | 1.82 (1.57, 2.12) | 2.00 (1.71, 2.33) | |||
| Zimbabwe | 2.15 (1.85, 2.47) | 2.54 (2.18, 2.97) | |||
| Income level | Low income | ||||
| Lower middle | 1.36 (1.17, 1.58) | 1.37 (1.17,1.60) | |||
| Random effect | |||||
| Variance | 43.38 | 38.42 | 34.25 | 29.12 | |
| ICC (%) | 47.45 | 38.52 | 32.32 | 16.43 | |
| MOR | 1.87 | 1.80 | 1.75 | 1.66 | |
| PCV(%) | Ref | 11.43 | 21.04 | 32.87 | |
| Model comparison | |||||
| Deviance | 6086.29 | 5856.580 | 5841.31 | 5835.23 | |
Measures of Variation
Discussion
Conclusion
Acknowledgments
Ethical Approval and Consent to Participate
Consent for Publication
Declaration of Conflicting Interests
Funding
ORCID iDs
Footnote
Data availability statement
Reference
Cite
Cite
Cite
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In

Keywords
Rights and permissions
Data availability statement
Authors
Authors’ Contributions
Metrics and citations
Metrics
Publication usage*
Total views and downloads: 1216
*Publication usage tracking started in December 2016
Altmetric
See the impact this article is making through the number of times it’s been read, and the Altmetric Score.
Learn more about the Altmetric Scores
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 3 view articles Opens in new tab
Crossref: 4
- Women's Health Dynamics in South Asia
- Association Between Decision-Making Styles, Personality Traits, and Socio-Demographic Factors in Women Choosing Voluntary Pregnancy Termination: A Cross-Sectional Study
- Married women’s autonomy in modern contraceptive utilization in Kutaber district, Northeast Ethiopia
- Prevalence and Factors Associated With Modern Contraceptive Use Among Orang Asli Women in Peninsular Malaysia: A Cross-Sectional Study
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Access journal content via a DeepDyve subscription or find out more about this option.
