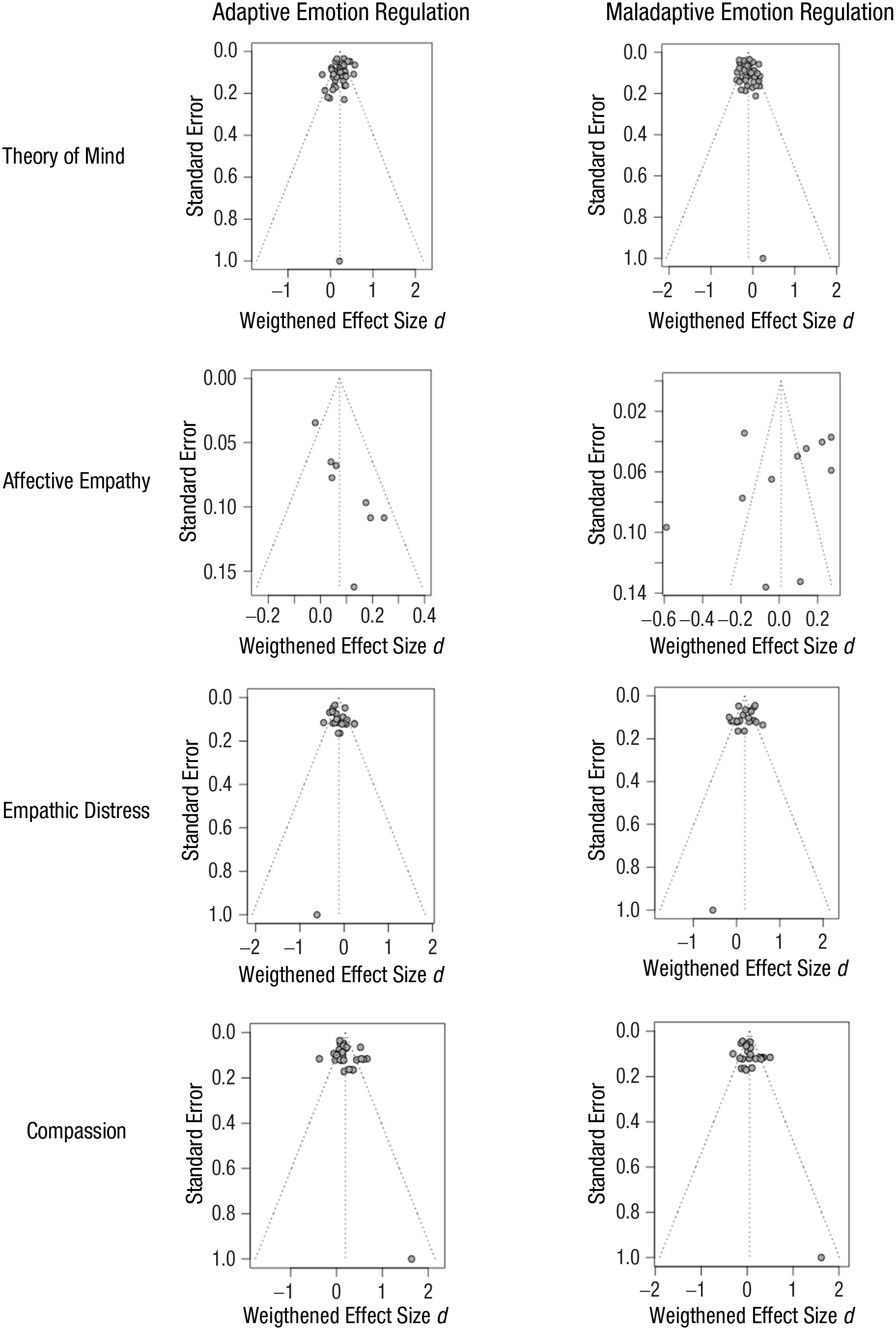
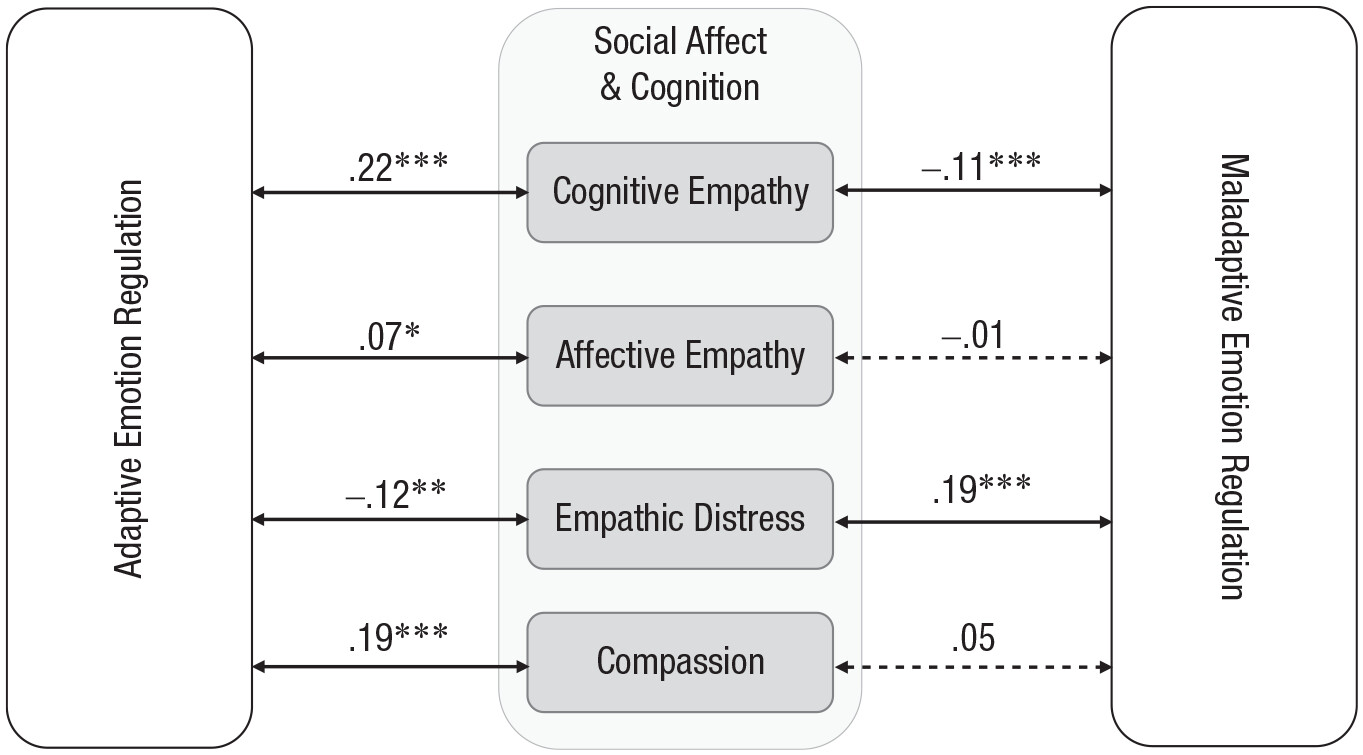
This meta-analysis provides a systematic summary of the state of research on the relationship between adaptive versus maladaptive emotion regulation and socioaffective and sociocognitive facets. We further sought to integrate evidence from clinical, developmental, intercultural, organizational, and personality psychology on this topic. Building on 42 studies (58 samples), the findings suggest that using adaptive emotion regulation positively relates to cognitive empathy, affective empathy, and compassion, whereas it negatively relates to empathic distress. Moreover, maladaptive emotion regulation is negatively related to cognitive empathy and positively related to empathic distress.
The relationship between emotion regulation and cognitive empathy
As expected, and consistent with prior work, our results showed a positive association between adaptive emotion regulation and cognitive empathy (e.g.,
Taute et al., 2010;
Wang et al., 2017) and a negative association between maladaptive emotion regulation and cognitive empathy (e.g.,
Lockwood et al., 2014). This is in line with theories from different areas of psychology (e.g.,
Eisenberg’s, 2010, theory of empathy-related responding;
Salovey and Mayer’s, 1990, concept of emotional intelligence; see also
Jordan et al., 2002): People who report being able to regulate their own emotions in an adaptive way are more likely to be able to take another person’s perspective, and people who report not being able to regulate their own emotions in an adaptive way are less likely to be able to take another person’s perspective. There are different possible explanations for this finding: Taking other people’s perspective might help to regulate one’s own emotions, for example, one might be less angry at the other person for making a mistake if one can also imagine that this person feels sad or ashamed because of the mistake. Another explanation could be that by being able to regulate one’s own emotions, one has the capacity to focus on the other person, which is a prerequisite for perspective taking. Cognitive empathy is resource demanding and requires both fluid and crystallized intelligence (
Ochsner & Gross, 2008;
Wieck et al., 2022); this finding shows that also regulating one’s emotions is inherently linked to accurately taking others’ perspective.
The negative association between maladaptive emotion regulation and cognitive empathy might also be explained by the focus of attention: For example, trying to suppress one’s feelings, rumination, or thinking about one’s past or future are self-centered emotion regulation strategies that might be associated with more difficulties focusing on other people’s perspectives. Furthermore, less cognitive empathy might also be part of not being able to react flexibly to the situation. This could be due to the use of a maladaptive strategy or difficulties fitting the right strategy to the situation (
Haines et al., 2016) because one might not be able to read the room or imagine how other people feel in a particular situation. This suggests that maladaptive emotion regulation interferes with cognitive empathy, whereas adaptive emotion regulation does not. Further, being less effective at regulating one’s feelings is related to anxiety, depressed mood, and stress (e.g.,
Garnefski & Kraaij, 2006;
Martin & Dahlen, 2005). In contrast, cognitive reappraisal, which is an adaptive regulation strategy, helps one to focus on other aspects of a situation, which thus helps to reframe the situation. This could imply that it facilitates focusing on the perspective of other people. Furthermore, our results could also mean that focusing on the perspective of other people seems to help to regulate one’s own feelings in an adaptive way. Future research could study the direction of the effect to investigate whether it is possible to shift focus from oneself to others by practicing more adaptive emotion regulation, to enhance, for example, leadership skills or reduce anxious or depressed symptomatology.
The relationship between emotion regulation and affective empathy
As expected, and in line with the findings of
Eisenberg and Fabes (1992), our results showed that adaptive emotion regulation and affective empathy were positively related (e.g.,
Taute et al., 2010), although the effect size was small. Surprisingly, in our meta-analysis, we found no link between maladaptive emotion regulation and affective empathy. However, we could include only nine studies investigating the link between affective empathy and adaptive emotion regulation and 11 studies investigating the link between affective empathy and maladaptive emotion regulation. Thus, the findings should be taken with caution. One possible explanation for both the small effect size for adaptive regulation and the nonsignificant effect for maladaptive regulation could be that the included studies differentially conceptualized and operationalized affective empathy, encompassing concepts such as mimicry, emotional contagion, and affective match (
Hess & Blairy, 2001). We were forced to combine these concepts given the small number of studies available, even though one might expect to find different results between more automatic, unconscious processes such as emotional contagion or mimicry and processes that might already involve emotion regulation, such as affective empathy or affective match. It is possible that automatic processes (e.g., contagion) occur too quickly or are unaffected by emotion regulation, whereas affective empathy is more intertwined with regulatory processes. Moreover, self–other differentiation is necessary for affective empathy, whereas emotion contagion is often considered a precursor of empathy that is already present in babies (
Singer & Klimecki, 2014).
Schipper and Petermann (2013) argue that affective empathy develops faster than cognitive empathy: Whereas affective empathy activates the amygdala, hypothalamus, and orbitofrontal cortex with fast processing of the emotion signal, cognitive empathy is more closely related to processes involved in executive functions and self-regulation. This is supported by the meta-analysis by
Yan and colleagues (2020), which showed that executive function was more strongly related to cognitive empathy (
r = .20) than to affective empathy (
r = .09).
In summary, less is known about the specific interactions between these differing conceptualizations of affective empathy and their specific timeline, and less research has been done regarding affective empathy and emotion regulation than regarding the other facets of the social affect and cognition. Accordingly, future researchers may wish to investigate these different processes (i.e., automatic vs. conscious processes) by combining different methodological approaches (i.e., implicit and explicit measures), complementing controlled laboratory sessions with experience-sampling studies, and looking from different perspectives (e.g., self- and other-report) in order to shed light on the specific timeline.
Other possible moderators
When different studies are included in a meta-analysis, the estimates will vary from one study to another. These differences might stem from random sampling error or from heterogeneity (
von Hippel, 2015). In our meta-analysis, there were several sources of heterogeneity, including differences in the measurement, the sample type, the study design, or the data-analysis method. Including such diverse studies made possible both an overview and a closer look at specific factors (different social affect and cognition facets or the type of measurement). Future research should further shed light on other possible mechanisms and moderators influencing the strength of the association between emotion regulation and different facets of social affect and cognition. For example, taking another person’s perspective or feeling empathetic with them may also be influenced by how that person has made someone feel previously, whether this person upset or cheered up his or her interaction partner, what kind of relationship they have with each other, or whether the person has sufficient resources and motivation to engage with the other person.
Furthermore, factors such as age and gender could also influence the way we regulate our emotions and our social affect and cognition. In their review,
Doerwald and colleagues (2016) describe that, compared with younger adults, older adults report being better at perceiving their emotions and having more cognitive empathy and more emotion regulation knowledge. However, the authors found no evidence for age differences between young and older adults’ effectiveness of regulating their own emotions. Other research has found that older adults show poorer performance in cognitive empathy than younger adults (e.g.,
Wieck et al., 2022) but perform at the same level or even better in affective empathy (
Sze et al., 2012;
Wieck & Kunzmann, 2015). However, the recent state of research does not reveal a clear picture, and findings are highly dependent on the method used. When using contextually embedded and age-fair tasks, age differences disappear (
Isaacowitz et al., 2017;
Wieck & Kunzmann, 2015). Future research could compare the different social affect and cognition facets between young and older adults, focusing on different methodological approaches.
As to gender,
Nolen-Hoeksema (2012) describes how women are widely viewed as more emotional than men, with greater tendencies to express their emotions, whereas men are pictured as tending to avoid both the experience and expression of emotions. Nolen-Hoeksema states that there are gender differences for self-reported rumination, with women generally reporting a higher tendency to ruminate than men, whereas
Berke et al. (2018) report that men are more externalizing (e.g., show aggressive behaviors) and suggest that these gender differences stem from childhood socialization and social pressure. It would be interesting to study how social affect and cognition is affected by socialization and whether the differences are reversible, for example, whether boys are explicitly being instructed to express their emotions.
In other words, both emotion regulation and social affect and cognition might depend on contextual (e.g., type of relationship, degree of resource demands) and individual (e.g., motivation, cognitive abilities, age, gender) factors, which should be investigated in future studies in more detail (
Thompson, van Reekum, & Chakrabarti, 2019;
Thompson, Uusberg, et al., 2019).
Theoretical and practical contributions
This meta-analysis makes several theoretical and practical contributions.
Pietromonaco and Collins (2017) found that both social connection and social disconnection shape biological responses and behaviors with consequences for one’s health and well-being. In this meta-analysis, we show that this link might be bidirectional: Our responses to our own emotions are also linked to whether we are able to connect to others (e.g., through compassion) or feel stressed by other people’s emotions (e.g., empathic distress). Accordingly,
Eisenberg (2010) suggested that emotion regulation contributes to a person’s ability to exhibit prosocial behavior (especially when there is a cost to the self). In this vein, the results of this meta-analysis point to possible theoretical explanations for why people who use maladaptive emotion regulation have smaller social networks and less satisfactory relationships (
Chervonsky & Hunt, 2017): They might perceive other people’s emotions as more overwhelming and stressful, making affective and cognitive empathy as well as compassion less likely and consequently leading to problems in their social lives. Moreover, not being able to put oneself in the shoes of others or feel compassion might affect whether one can choose the most adaptive strategy in a situation (
Haines et al., 2016).
Social relationships play a crucial role in our everyday lives and in our well-being (
Pietromonaco & Collins, 2017). Connecting personal strategies of emotion regulation to how we react to other people’s emotions, and hence understanding specific mechanisms of social affect and cognition, offers new potential avenues for interventions to reintegrate people into social contexts. Various therapeutic approaches already incorporate emotion regulation training (
Aldao et al., 2010), including dialectical behavioral therapy (
Linehan, 1987) and emotion regulation therapy (
Mennin & Fresco, 2014). However, this meta-analysis indicates that the effect of such interventions on patients’ social relationships might be bigger than expected, as emotion regulation affects the social affect and cognition in various ways. This finding could have practical implications for therapeutic approaches, as it shows that patients might show improvements in interpersonal behavior after learning adaptive emotion regulation.
Limitations and future directions
Both social affect and cognition and emotion regulation are multidimensional constructs, and they were defined and operationalized in different ways in the included studies. This may have led to conceptual blurriness with respect to cognitive and affective empathy, as demonstrated by the fact that we had to subsume different concepts (for cognitive empathy: perspective taking, theory of mind, mentalizing, empathic accuracy; for affective empathy: emotion contagion, affective match) under this term. This blurriness probably affected our results. Less research has been done regarding the link between emotion regulation and affective empathy. This might be because of the aforementioned blurriness of the concept but also because of difficulties in eliciting authentic emotions worth regulating in the laboratory. It therefore seems necessary to develop a concise definition but also to conduct more studies using real-life interactions, such as couple studies in the laboratory (e.g.,
Haase et al., 2016;
Rohr et al., 2019) or ecological momentary assessments conducted in vivo (e.g.,
Colombo et al., 2020). Future researchers should seek to close this gap in order to gain further insights into how emotion regulation might affect the perception of social contexts (via social affect and cognition), how this might be connected to mental disorders, and how people actually behave in social contexts.
The same is true for empathic distress, which is used to describe a multitude of stressful experiences that can vary depending on the situation. Moreover, our meta-analysis indicates that some measures of emotion regulation overlap with psychopathology measures (
Treynor et al., 2003); for example, rumination is not only a form of maladaptive emotion regulation but also a part of depressive symptomatology. Finally, clinical models of emotion regulation are distinct from prominent models of emotion regulation in basic affective science (e.g.,
Gross, 1998). Whereas those frameworks tend to conceptualize emotion regulation as more process-oriented, clinical psychology defines emotion regulation more as an ability that can be trained and developed, and difficulties in emotion regulation are seen as an important maintaining factor of mental disorders (
Hallion et al., 2018). Furthermore, researchers have recently proposed dynamic models of emotion regulation in which various factors interact (e.g., demographic variation, personality, type of emotion, sensitivity to context, availability of a diverse repertoire of regulatory strategies, responsiveness to feedback, timing;
Bonanno & Burton, 2013;
Chen & Bonanno, 2021), which because of sample size could not be investigated as different factors. Because we included emotion regulation questionnaires that differ in their conceptual backgrounds, we could include a much broader range of studies. However, the Self-Report Instrument for the Assessment of Emotion-Specific Regulation Skills (
Ebert et al., 2013), the Emotional Competence Questionnaire (Rindermann, 2009), or the Emotion Regulation Inventory (
König, 2011), measure emotion regulation competencies in a way that is emotionally specific and/or competence oriented, whereas other research has focused on assessing difficulties in emotion regulation, such as the Cognitive Emotion Regulation Questionnaire (
Garnefski & Kraaij, 2007) or the DERS (
Gratz & Roemer, 2004). Those questionnaires have their roots in clinical psychology, more concretely “in ‘third-wave’ models of cognitive behavioral therapy, which propose a central role for experiential avoidance in the onset and maintenance of most forms of emotional disturbance” (
Hallion et al., 2018, para. 1). The most widely used questionnaire, the ERQ (
Abler & Kessler, 2009;
Gross & John, 2003), assesses the frequency of different strategies used. We divided scales and subscales of these different questionnaires into adaptive and maladaptive emotion regulation. This enabled us to include data from other areas of psychology and consequently gain a broader overview, but this was also limited by the use of a categorical system—it did not reflect the complexity of everyday life. A strength of our study was that we included studies from all areas of psychology, leading to a haziness in understanding the process level of the interplay between regulatory and social affective and cognitive processes. Future studies in clinical psychology focusing on more recent multicomponent models of emotion regulation, which take into account context sensitivity, repertoire, and feedback responsiveness (
Chen & Bonanno, 2021) or goals (
Millgram et al., 2020), might offer new insights on the interplay between mental disorders and social affect and cognition. Overall, it would be fruitful for future research to develop consistent and precise definitions by combining and comparing different theoretical approaches and testing the suitability of different methodological approaches to measure these precise definitions.
Furthermore, most of the studies included in this meta-analysis relied on self-report data, especially regarding the assessment of emotion regulation, where only one measurement (the Mayer-Salovey-Caruso emotional intelligence test; see
Table S1) was performance based. Previous research has shown that behavioral and self-report data often yield different findings regarding the relationships between, for example, affective empathy and depression (
Schreiter et al., 2013). In other words, it is not clear whether individuals accurately report their emotion regulation strategies and social affective and cognitive abilities (
Robinson & Clore, 2002), as this requires metacognitive abilities and might be influenced by moods, social desirability, or self-presentation biases. For example, people with social anxiety underestimate their social abilities (
Hofmann, 2007). Furthermore, often-used measures such as the ERQ are limited to two emotion regulation strategies (reappraisal and suppression) and assess only the frequency of use and do not include the fit of a certain strategy for a situation (
Haines et al., 2016). Therefore, one avenue for further research is more performance-based studies comparing different situations, as self-reports do not necessarily predict how people act in a real-life situation. One challenge of performance-based research is to develop stimuli that are able to evoke emotions in the study participants (
Wieck et al., 2022). In this vein,
Eisenberg (2010) suggests that if an empathy-inducing stimulus is not potent enough to elicit emotions in the observer, emotion regulation may be irrelevant. Newly developed test-based measures that evoke emotions tackle this issue, for example, with video clips depicting people talking about an emotional situation and expressing emotions (e.g.,
Kanske et al., 2015;
Wieck & Kunzmann, 2015;
Wieck et al., 2022).
This meta-analysis was intended to provide an overview of the current state of research; however, an overarching theory on the relationship and processes linking emotion regulation and social affect and cognition is still missing.
Thompson, Uusberg, et al. (2019) suggest a framework for empathy and emotion regulation processes by stating that real-world interactions encompass complex dynamics between perception, mimicry, and cognitive processes, where both interaction partners influence each other to a degree that depends on their capacity and propensity to do so.
Schurz and colleagues (2021) propose a hierarchical model of social cognition, similar to models of intelligence research, with predominantly cognitive processes, more affective processes, and combined processes. However, the studies included in this meta-analysis are correlational; hence, no claims of directionality or processes can be made. To shed light on the timeline of emotion regulatory and social affective and cognitive processes within interpersonal interaction, more studies with different methodological approaches are needed. For example, it might be fruitful for future studies to analyze the interplay between these processes on the individual level (e.g., social affective and cognitive processes, emotion regulation abilities, motivation) and social level (e.g., similarity between interaction partners). For instance, there are at least three potential explanations for a person experiencing compassion: (a) People differ in their tendency to be compassionate toward others (actor effect), (b) people vary in their tendency to elicit compassion (partner effect), or (c) the person who feels compassion for the other person has a specific compassionate relationship with the other person; in other words, people differ in their specific compassionate match (relationship effect). Another avenue of research could be to investigate whether people differ in their level of compassion depending on the situation or to make a detailed analysis of the different parts that encompass adaptive emotion regulation (e.g., flexibility, repertoire, frequent use of a certain strategy). Further follow-up questions could be to investigate the factors that facilitate social affective and cognitive matches, such as processes of emotional coregulation (
English & Eldesouky, 2020) or similarity. Methodological approaches, such as the social-relations model by
Back and Kenny (2010), might lead to more profound insights on the interplay between emotion regulation and social affect and cognition.
Furthermore, we did not account for contextual influences on emotion regulation and social affect and cognition, such as how these processes differ between different emotions (e.g., anger, sadness or happiness), interpersonal relationships (e.g., coworkers or romantic partners), or cultural contexts.
Haga and colleagues (2009), for example, found differences in the use of strategies across cultures, ages, and gender. This meta-analysis relies mostly on data from Western adult cisgender males and cisgender females in the laboratory, which might not be representative of the interplay between emotion regulation and social affect and cognition in general. Rather, it reflects how these processes can be typically observed in these specific groups in individualistic countries.