Introduction
Playing musical instruments is associated with long-term health benefits (see the review by
Dingle et al. (2021)). Yet, music-making, whether pursued at an amateur or professional level, may also pose inherent risks, including the potential for developing noise-induced hearing impairments (
Musgrave, 2022;
Schink et al., 2014). The likelihood of developing such impairments is influenced by the duration and intensity of noise exposure: both short but intense noise levels of 137 dB
peak-C, as well as comparatively low but prolonged exposure at an average of 85 dB-A over several years, have been reported to result in permanent noise-induced hearing loss (HL) (
Liedtke, 2010; “Königsteiner” and “NIOSH” recommendations;
Chan, 1998;
Deutsche Gesetzliche Unfallversicherung, 2013,
2020). Indeed, musicians regularly confront sound intensity levels that not only challenge but also endanger their hearing (
O'Brien et al., 2013). Depending on their instrument, position, and repertoire, they often face peak sound levels of up to 135 dB-C and practice durations extending to 6 hours daily (
Halevi-Katz et al., 2015;
Rodrigues et al., 2014;
Schmidt et al., 2011). Consequently, bound to their profession, musicians are inherently at risk for developing noise-induced hearing impairments (
Gong et al., 2018;
Schink et al., 2014).
A body of research highlights the risks musicians face in terms of hearing health.
Phillips and Mace (2008) report that 48% of music students are exposed to harmful noise levels during daily practice. Similarly,
O'Brien et al. (2013) found that 53% of musicians surpass the permissible daily noise exposure limits (see also
Tufts & Skoe, 2018), a salient finding, as it does not include time spent in orchestral rehearsals and concert performances (i.e., only solitary practice was considered). It is therefore not surprising that
Halevi-Katz et al. (2015) linked greater musical experience (years of persistent music playing) to higher hearing thresholds in the frequency range of 3–6 kHz. Furthermore,
Hasson et al. (2009) reported that 40% of musicians experience some form of hearing disorder, with tinnitus (19%) being the most common, followed by 14% suffering from hyperacusis (one form of auditory hypersensitivity), and 6% experiencing difficulties in noisy environments or sound distortions—a finding that is consistent with
Harper (2002), who recorded hearing problems among 38% of British and 37% of German musicians. Notably, a systematic review by
Di Stadio et al. (2018) revealed that professional musicians in pop/rock genres are at an even higher risk of developing HL and other audiological symptoms compared to classical musicians.
Gembris et al. (2018) further indicated that the likelihood of hearing problems of orchestra musicians escalates with age. The impact of HL extends beyond listening abilities, affecting mental health and social well-being.
Bigelow et al. (2020) demonstrated that HL correlates with increased psychological distress, greater use of antidepressants, and higher dependency on mental health services among the general population.
However, the relationship between noise exposure and hearing impairment is not always straightforward. For example,
Prendergast et al. (2017) had difficulties relating noise exposure to perceptual deficits in young listeners (mostly nonmusicians) with normal hearing (NH) audiometry.
Couth et al. (2020) investigated this in a sample of musicians but could only find subclinical effects of noise exposure on hearing. Moreover,
Russo et al. (2013) found no significant differences in hearing issues between instrument groups, even though brass, woodwinds, and percussionists have been reported to be exposed to particularly high sound levels (e.g.,
Rodrigues et al., 2014;
Schmidt et al., 2011).
In summary, musicians commonly face hearing health challenges such as HL and tinnitus, impacting their musical performance and overall quality of life (
Halevi-Katz et al., 2015;
Hébert & Lupien, 2009;
Richter, 2011). Furthermore, hearing health may directly and indirectly affect the ability to perceive, appreciate, and produce music, alongside impacting mental, physical, and social well-being (e.g.,
Bigelow et al., 2020;
Gembris et al., 2018,
Musgrave, 2022;
Scherer, 2004,
Zentner et al., 2008).
Recognizing the risks to hearing health in musicians, it becomes crucial to focus on their habits and preventive strategies. Certainly, adopting behaviors that reduce exposure to loud noise is essential for preventing hearing problems (e.g.,
Hébert & Lupien, 2009;
Olsen et al., 2016;
Richter, 2011). Intervention strategies for public health thus often include the promotion of hearing protection (e.g.,
Occupational Safety and Health Administration, 2002). Still, the actual usage of hearing protection among musicians and the barriers to its consistent application remain key concerns.
Laitinen (2005), for example, found that among classical musicians in Finland, the use of hearing protection is sporadic, often commencing only after the onset of auditory symptoms. Specifically, a mere 6% consistently use hearing protection, while 35% seldom do—despite the fact that 31% reported some form of HL and 37% reported experiencing tinnitus. However, these are not uniformly distributed across regions. Among Australian musicians, 40% reported using hearing protection during practice, and 64% claimed occasional earplug use (
O'Brien et al., 2013,
2014). This contrasts with orchestras in Germany, where only 38% reported occasional hearing protection use (
Zander et al., 2008). Interestingly, there is some indication that younger musicians are more inclined toward protective measures: a study by
Couth et al. (2021) found that among 80 British early-career musicians, 77% used hearing protection at least once a week.
The inconsistent use of hearing protection among musicians, despite the well-documented risks, demands an examination of the motivations behind these unhealthy choices. This exploration must consider the significant role of awareness in shaping health-related behavior. While awareness is often a precursor to behavioral change (e.g.,
Ajzen, 1991), one might assume that greater awareness of hearing health risks among musicians would naturally lead to increased use of hearing protection. For instance, studies by Keppler et al. (2015a, 2015b, 2015c) suggest that increasing awareness about hearing health substantially contributes to the adoption of protective measures against recreational noise. However, this inference is complicated by findings from
Laitinen (2005), where a very high percentage (94%) of musicians reported concern for their auditory health, yet the actual use of hearing protection was notably low (6% consistent usage). This disparity suggests the presence of other barriers within the musical context, which may be intrinsic to the professional demands and social dynamics of musical performance. For example, musicians frequently cite issues with sound quality and difficulties hearing other musicians as significant obstacles to consistent hearing protection use (
Laitinen, 2005;
O'Brien et al., 2014;
Zander et al., 2008). Additional factors such as varying loudness levels during performances or hampered self-monitoring could further discourage musicians from using hearing protection. Moreover, there is a less explored but equally compelling aspect that may hinder the consistent use of hearing protection among musicians—concerns about one's professional image. The use of hearing protection could potentially be perceived as a sign of auditory weakness, thereby affecting a musician’s reputation or audience perception (see
Couth et al., 2021).
A similar dynamic may also contribute to the reluctance toward hearing aid adoption. Despite their proven utility in enhancing auditory experiences, hearing aids remain underutilized (e.g.,
Chern et al., 2023). While the literature does not specifically address the potential impact on musicians’ reputation as a factor in hearing aid adoption, musicians repeatedly complain that devices often are not effectively equipped or fitted to account for the full dynamics essential in music (e.g.,
Madsen & Moore, 2014). Recently,
Greasley et al. (2020) extensively explored the complex dynamics of hearing aid usage among musicians by considering both audiologists’ and patients’ perspectives in the UK. Their study revealed another factor: a significant misalignment in expectations and understanding between these groups. Among musicians who use hearing aids, only 42% report an enhanced enjoyment of music while wearing them, with half experiencing distortions and over two-thirds encountering problems occasionally. A primary concern is the gap in audiologists’ training and understanding regarding the specific demands of hearing aids in musical environments. Only a small proportion (37%) of audiologists have received training focused on music, and despite 74% seeking additional information on this subject, many still express only moderate confidence in advising patients about music and hearing aids. Indeed, 58% of patients reported that music listening was never discussed. Consequently, many musicians feel their unique needs for high-quality music listening are not being met, leading to dissatisfaction and low adoption rates. These insights underscore a need for more specialized knowledge and tailor-made solutions in hearing aids for musicians. While awareness is a critical factor, it does not operate in isolation. The limited adoption of hearing protection and hearing aids is a complex interplay of personal, professional, and societal factors, warranting a multifaceted approach to intervention.
In sum, the literature suggests a link between musical noise and an increased risk of hearing problems in musicians, yet generalizing these findings across different groups and levels of exposure remains challenging. Existing studies predominantly focus on professional musicians, disregarding the large proportion of recreational (amateur) musicians—which amount to 14.3 million musicians in Germany alone (
Deutsches Musikinformationszentrum, 2021). This necessitates a more detailed investigation into how music-related noise exposure affects musicians, particularly considering the varied intensity levels associated with different instrument groups, the range of environments in which music is performed (from individual practice at home to full orchestral performances), and the frequency and duration of musical activities (that is, considering both professional and amateur musicians). Despite this, the literature provides limited insight into the specific requirements necessary to implement preventive measures effectively. This gap extends to understanding how awareness and concerns about reputation influence musicians’ decisions, particularly regarding the use of hearing protection and the adoption of hearing aids.
The Current Study
Addressing this gap, the current study aimed to provide a comprehensive investigation of hearing health among orchestral musicians, both professional and amateur. This included examining the utilization of and attitudes toward hearing protection and hearing aids, the prevalence and types of hearing problems, and their overall impact on musicians’ well-being. While the analysis was exploratory in nature, it was underpinned by two primary hypotheses: Professional musicians were expected to (a) report more hearing problems and (b) demonstrate a higher level of awareness toward hearing health compared to their amateur counterparts. Additionally, this research aimed to delve into the usage, experiences, and effectiveness of various strategies employed to protect hearing health. An important facet of this exploration was to identify and analyze the key factors that influenced the adoption rates of hearing protection and hearing aids among musicians. Subsidiary to these main goals, the study also explored the influence of demographic factors, specifically age as a critical factor in HL, on these relationships.
Results
Musician Group Matching
Unmatched groups in comparative analyses can introduce significant bias due to confounding variables, thereby undermining the internal validity of the analysis. To probe for preexisting differences between professional and amateur musicians, a Chi-square test of independence was conducted, showing an significant association between group membership (amateur vs. professional) for age,
χ²(7) = 133.6,
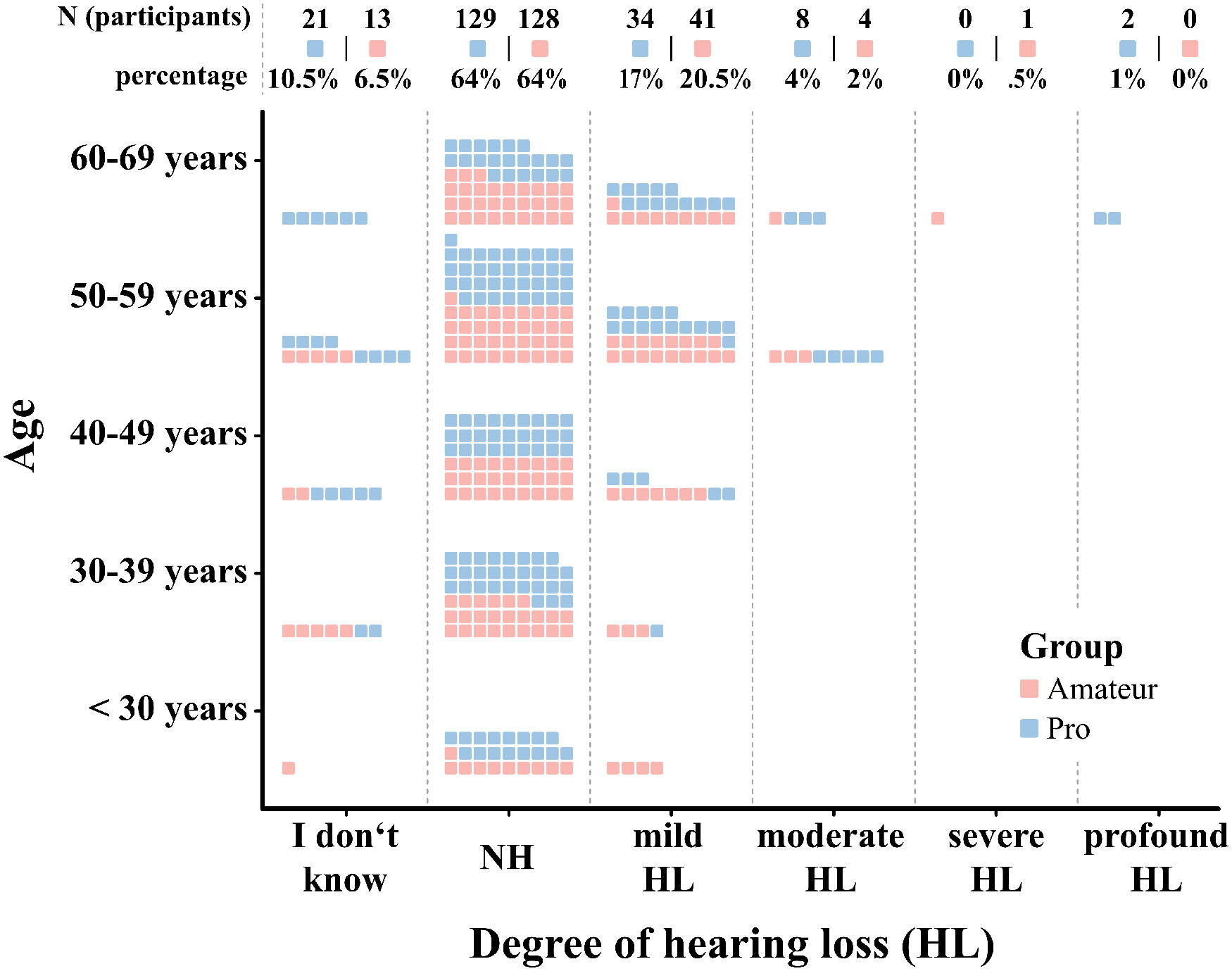
p < .001. Upon further inspection it became apparent that comparably few young (up to 30 years) and senior professional musicians (70 years and above) participated in the survey compared to the amateurs (see
Figure 1A). Similarly, there were significant differences between group membership for gender,
χ²(3) = 8.3,
p = .004, and for participants instrument family, χ²(5) = 23.5,
p < .001 (see
Table A3 in Supplementary Materials for the grouping of instruments). Thus, participants’ musical group membership (professionals vs. amateurs) demonstrated imbalance across age, gender, and instruments family.
In order to mitigate confounding effects, a matching algorithm was applied, utilizing the
MatchIt package (v4.5.3;
Ho et al., 2007). This package serves as a statistical tool designed to ensure comparability between professional musicians and amateurs by balancing the participant groups on several key demographics: age, gender, and instrument family of their primary (contract) instrument. A combination of the “optimal” and “exact” matching procedures was applied. The most critical aspect of this approach was the exact matching on age, since it significantly influences hearing. This method ensured that each pair of participants—comprising one professional and one amateur musician—was matched “exactly” within the same age group. For the variables of gender and instrument family, the “optimal” matching method was selected, coupled with the “Euclidean” distance metric. Rather than matching each pair precisely, this strategy aimed to minimize the overall distance across pairs in these two dimensions. Essentially, the result is a subsample in which each professional musician was balanced strictly in terms of age, with a more flexible distribution for gender and instrument family. This method allowed for a more nuanced matching, taking into account the combined effects of age, gender, and instrument family, while ensuring that a sufficient number of participants are retained for subsequent analysis.
After matching, 82 unmatched subjects from the professional musician group, and 113 from the amateur group were excluded. Accordingly, a total of 400 participants remained for the analysis. The distributions for age, gender, and instrument group before and after matching are represented in
Figure 1. In conclusion, the matching process successfully balanced the key variables of age, gender, and instrument family between the professional and amateur musicians. That is, there are no statistically significant differences between groups neither in age,
χ²(4) = 0,
p = 1, gender,
χ²(3) = 1.3,
p = .73, and instrument group,
χ²(5) = 1.27,
p = .94, after matching. It is critical to note that despite the improvements in balance across these variables, other imbalances remained post-matching, for example, in repertoire played by the orchestra (see
Figure A2 in Supplementary Materials). The demographic distribution of the final sample closely mirrors that of professional musicians in Germany, with deviations from the reference populations remaining within a 5% proportional margin. Thus, the sample presented here can be regarded as representative (see
Versorgungsanstalt der deutschen Kulturorchester, 2021).
Hearing-Related Problems
Participants who had received professional audiometric evaluations were instructed to report the final results of those assessments, specifically indicating whether they had been diagnosed with mild, moderate, severe, or profound HL. For participants who had not undergone professional audiometric assessments in the past and were thus unaware of their specific degree of HL, they were instructed to self-estimate their HL. Almost all professional musicians stated to have their hearing checked (97%), whereas only 72% of amateurs had their hearing checked by a professional at least once before. On average, the last appointment was 2.7 years ago (SD = 3.8) for professionals and 5.2 years (SD = 6) for amateurs.
Both self-estimated and self-reported results of professionally diagnosed HL were included in the analysis. Overall, 22% of professionals (
N = 44) and 23% of amateurs (
N = 46) reported having at least a mild form of HL (see
Figure 2). In addition, 24% of musicians (23.3% amateurs, 24.7% professionals) reported having tinnitus, 49.1% (44.8% amateurs, 53.3% professionals) reported being oversensitive to high sound levels, and 15.9% (11.9% amateurs, 18% professionals) reported other hearing problems. There were no significant differences of reported hearing problems across groups (professionals vs. amateurs) for the degree of HL, χ²(1) = 4.1,
p = .26, tinnitus,
χ²(1) = 1.84,
p = .22, oversensitivity,
χ²(1) = 2.87,
p = .1, or reporting other problems, χ²(1) = 2.8,
p = .12. Taken together, two-thirds (66.75%) of the respondents reported experiencing at least one of these kinds of hearing problems—a pattern that is indifferent to the musician’s group membership, with 67.5% of amateurs and 66% of professionals affected. Similarly, employing the HDDA HL screening cutoff (<18 indicating mild impairment;
Jacob et al., 2017), a total of 107 individuals (48 amateurs, 59 professionals) were classified as hearing impaired. A chi-squared test found no significant difference in this classification between the groups,
χ²(1,
N = 385) = 1.37,
p = .242, further suggesting that the proportion of individuals with hearing difficulties may be similar across both groups.
Furthermore, the analysis did not suggest any significant difference in the MRHP scale between the groups of musicians, Mdn
diff. = .24;
W = 18554,
p = .3,
rrb (rank biserial) = .06, 95% CI [−.06, .18]; see
Figure 3. Differences were observed, however, in the HDDA scale between the musician groups. Professional musicians reported more problems in social interaction (Mdn = 12, MAD = 4.45), compared to amateur musicians (Mdn = 13, MAD = 2.97). Lower scores indicate more severe hearing problems. The Wilcoxon rank-sum test revealed this difference to be statistically significant,
W(391) = 21,519,
p = .03. The effect size was
rrb = .13, indicating a negligible effect. There were no statistically significant differences between the groups in the HDDA subscale for basic sound perception,
W(391) = 14,300,
p = .59.
Influence of HL and Age
When conducted irrespective of musicians’ group membership (also excluding “I don’t know” responses), a Kruskal–Wallis test indicated statistically significant differences in MRHP scores across the participants’ degree in hearing-impairment,
H(2, 374) = 27.4,
p < .001, with a subtle effect size (
ε² = .07; see
Figure 3). The median MRHP factor score was 1.14 (MAD = 1.7) for musicians with NH, 1.61 (MAD = 1.8) for the “mild hearing loss” (mild HL), and 4.23 (MAD = 1.5) for the “at least moderate HL” (moderate HL). A post-hoc pairwise Wilcoxon rank-sum test revealed that the differences were significant between the “NH” and the “mild HL” (
p = .02), between the “NH” and the “at least moderate HL” (
p < .001), as well as between the “mild HL” and the “at least moderate HL” group (
p = .001). Likewise, HDDA scores showed significant effects with the reported degree of HL. The Kruskal–Wallis test revealed significant variance across the HL types,
H(2, 391) = 100.4,
p < .001, with a moderate effect size (
ε² = .27). The Wilcoxon post-hoc test confirmed significant differences between all groups, that is, “NH” (Mdn =14, MAD = 3) and both “the mild HL” (Mdn = 9, MAD = 3) and “at least moderate HL” (Mdn = 6, MAD = 1.5), and also between the latter two (all comparisons reach
p < .001).
No statistically significant differences were found for participants’ MRHP scores between age groups, H(4, 359) = 3.23, p = .52. In contrast, significant age-related differences were observed in the HDDA subscore for social interactions, H(4, 400) = 23.2, p < .001, although the overall effect size was marginal (ε² = .06). Post-hoc analysis revealed statistically significant differences between the “below <30” (Mdn = 14, MAD = 3) and “50–59” age groups (Mdn = 11, MAD = 3; p = .03), as well as between the “30–39” (Mdn = 14, MAD = 3) and both the “50–59” (p = .001) and “60–69” (Mdn = 12, MAD = 4.5, p = .007) age groups. No other age group comparisons yielded statistically significant results.
Use of Hearing Protection
Overall, a majority of participants (59.4%,
N = 240) acknowledged that playing music poses a risk to their hearing health due to the exposure to high sound levels; however, merely 52% of those who recognized the risk chose to wear any hearing protection. More strikingly, over 35% of respondents who affirmed the statement (respond with “true”)—“
The sound levels in the orchestra are so high at times that I should wear ear protection”—and 77% of those who concurred with “rather true”, abstained from using hearing protection all together. In group comparisons, professionals exhibit a markedly higher tendency to use hearing protection compared to their amateur counterparts (53.5% of professionals vs. 12% of amateurs). However, the majority of musicians reported rarely or never using hearing protection, with percentages ranging from 72.5% to 82.4% for amateurs and from 14.5% to 70.6% for professionals, depending on the playing context (Detailed statistics are provided in
Table 1). Notably, only 4% of professional musicians reported always using hearing protection during individual practice, compared to .5% of amateurs. This discrepancy widens during rehearsals, with 9.9% of professionals versus 0% of amateurs always using hearing protection. The trend persists during concerts, where 10.4% of professionals and only 1.5% of amateurs consistently use hearing protection. By combining reported hearing protection usage with individuals’ total instrumental playing time (similar to the method used for estimating the probability of attenuation in the UNE), it was found that amateurs spent 79.5% of their playing time unprotected, 19.5% partially protected (e.g., using protection in one ear or occasionally removing it), and 1% fully protected. In contrast, professional musicians spent 34% of their playing time unprotected, 57% partially protected, and 9% fully protected.
When examining the consistent use of hearing protection in conjunction with the degree of HL, a significant trend was observed, H(2, 364) = 13.25, p = .001. Specifically, analyzed irrespective of musicians group membership, 3% (SD = .15) of respondents with NH always used hearing protection. This percentage increased to 5% (SD = .19) among those with mild HL and surged to 22% (SD = .36) among individuals with at least moderate HL. Post-hoc pairwise Wilcoxon rank-sum tests revealed significant differences between those with at least moderate HL and mild HL (p < .001), as well as between those with at least moderate HL and NH (p = .03).
Noise Exposure
Professional musicians reported significantly higher practice and performance durations than their amateur counterparts. On average, professionals engaged in 7.1 hours (SD = 4.2) of weekly practice for concerts, whereas amateurs reported an average of 8 hours (SD = 1.4). Rehearsal times followed a similar pattern, with professionals practising 15.2 hours weekly (SD = 5.9), in contrast to 3 hours (SD = 2.3) for amateurs. Besides group performances, professionals also practised more (i.e., individual practice), averaging 8.6 hours per week (SD = 5.1) compared to amateurs’ 3.6 hours (SD = 3.7).
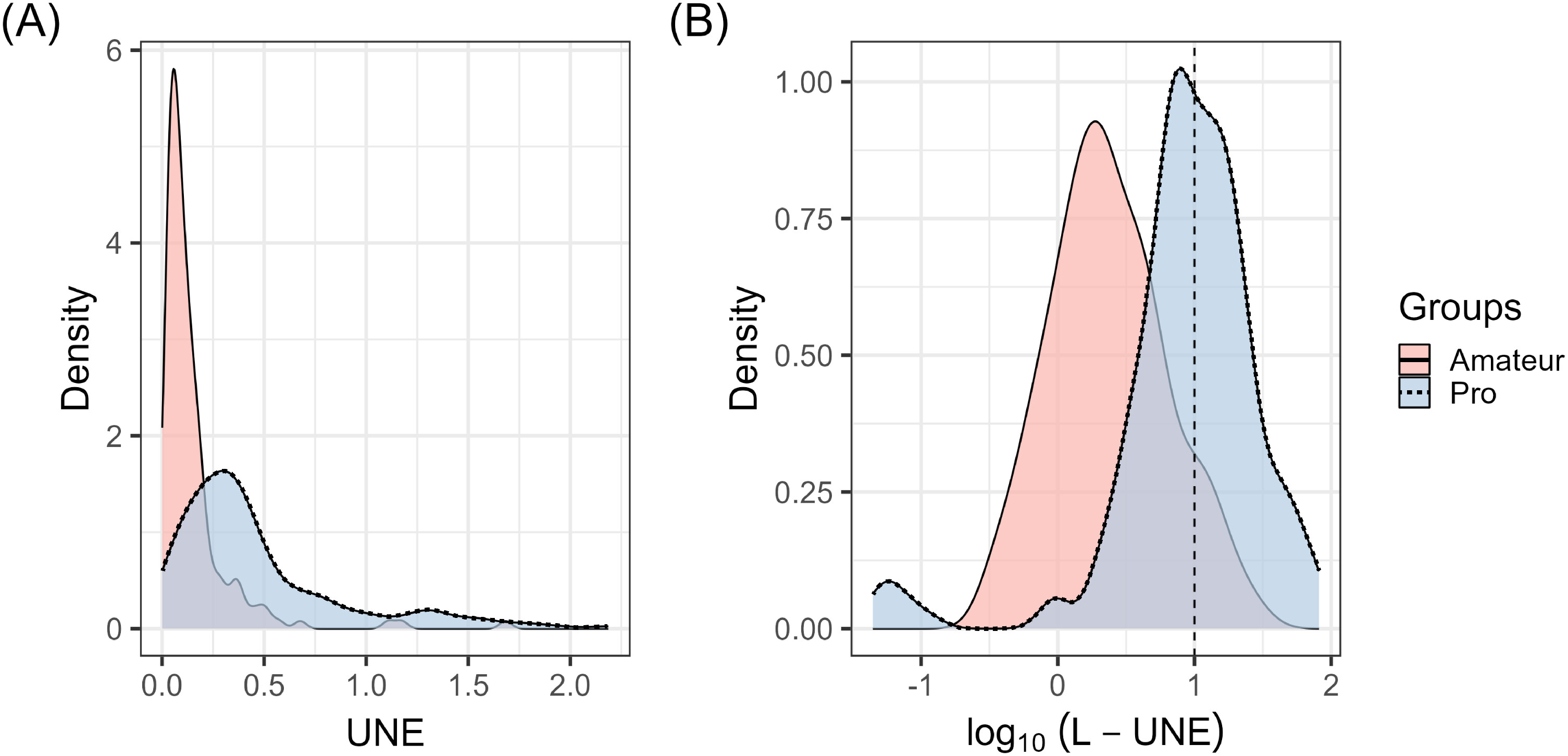
Based on these practice habits, instrument groups, and hearing protection usage, participants’ self-reported musical UNE was derived. Following the classification by
Prendergast et al. (2017), individuals with a log
10(L-UNE) of one or higher were categorized as having high noise exposure—equivalent to a decade of exposure at 90 dB-A. According to this criterion, a proportion of 50% of professional musicians were classified within the high noise exposure group, a figure that contrasts with the 9.9% of amateur musicians, as illustrated in
Figure 4.
In addition, the Wilcoxon rank-sum test revealed significant group differences in UNE and L-UNE: Professional musicians registered almost three times higher median levels of musical sound exposure (UNEMdn = .34, MAD = .25) and almost four times higher lifetime music noise exposure (L-UNEMdn = 10, MAD = 8.1), relative to their amateur counterparts, who reported lower levels of UNEMdn = .09 (MAD = .07) and L-UNEMdn = 2.1 (MAD = 1.91). These differences were statistically significant for both UNE, W(364) = 5828, p < .001, and L-UNE, W(364) = 5291, p < .001. The effect sizes were considerable, with rrb = −.65, 95% CI [−.71, −.57] for UNE and rrb = −.68, 95% CI [−.74, −.61] for L-UNE. Notably, 57% of amateurs’ lifetime music noise exposure have been experienced during individual practice, 33% during rehearsals, and 10% during concerts. In contrast, professionals experienced 49.4% during practice, 34.2% during rehearsals, and 16.4% during concerts.
Influence of HL and Age
In examining the association between UNE and age, the following pattern emerged: UNE was found to be highest among the youngest participants, with those under 30 years showing a median UNE score of .35 (MAD = .34). Overall, the UNE score decreased with age, reaching its lowest values in the 40–49 age group, with a median score of .14 (MAD = .16), and remaining that low for the rest of the musician’s career (see
Figure A3 in Supplementary Materials). This effect was statistically significant,
H(2, 364) = 23.2,
p < .001, demonstrating a marginal effect size (ε² = .04). Post-hoc analyses utilizing pairwise
t-tests revealed that the “below 30” age group is significantly higher when compared with the “40–49” (
p < .01), the “50–59” (Mdn = .16, MAD = .17,
p < .01), and “60–69” (Mdn = .18, MAD = .19,
p = .04) age groups. With respect to the degree of HL, no significant differences were observed—neither for the UNE,
H(2, 364) = .58,
p = .75, nor the L-UNE,
H(2, 364) = 1.02,
p = .6.
Hearing Health Awareness
In the present study, musicians generally perceived hearing health as a topic that does not receive enough discussion, with 71.5% affirming this view as either “rather true” or “true”. This sentiment was slightly more common among amateurs (78.5%) compared to professionals (64%). Furthermore, a significant majority (74.75%) expressed a desire for regular counselling on the topic of hearing health and hearing impairment (at least “rather true”), with a higher interest demonstrated by professional musicians (81.5%) compared to amateurs (68%). However, a quarter of respondents (24%) expressed reluctance, responding with “not true” or “rather not true” when asked if they would discuss their HL openly. These rather negative attitudes toward hearing health were further reflected in the HHA factor scores. Overall, amateur musicians exhibited lower average awareness scores (HHA
Mdn = 4.1, MAD = 3) compared to professional musicians (HHA
Mdn = 8.1, MAD = 1.3). This difference was statistically significant,
W(359) = 5711,
p < .001, with a very strong effect size (
rrb = −.65, 95% CI [−.71, −.6]), suggesting a substantial difference in HHA between amateur and professional musicians (see also
Figure 5).
Influence of HL and Age
The HHA factor scores also revealed significant differences across HL categories,
H(2, 359) = 9.4,
p = .01; see
Figure 5B. The NH group had a median HHA score of 6.2 (MAD = 3.3), the “mild HL” group 7.1 (MAD = 2.4), and the “at least moderate HL” group 8.3 (MAD = 1.4). However, the effect size was rather small (ε² = .03). The corresponding post hoc test found only the difference between the “NH” and “at least moderate HL” group in HHA scores to be statistically significant (
p = .03). In terms of age, no differences in HHA factor scores could be observed,
H(4, 359) = 3.2,
p = .52.
Hearing aid Disapproval
The analysis of the HAD scale revealed significant differences in approval ratings between amateur and professional musicians. Professional musicians exhibited higher levels of disapproval toward hearing aids (HAD
Mdn = 6, MAD = 3.2) compared to their amateur counterparts (HAD
Mdn = 2.6, MAD = 3.9; see
Figure 5). This difference was statistically significant,
W(335) = 9584.5,
p < .001, and demonstrated a moderate effect size,
rrb = −.32, 95% CI [−.42, −.2].
Influence of HL and Age
Moreover, the data indicated a relationship between age and HAD scores, with the Kruskal–Wallis test showing statistically significant differences and a small effect size,
H(4, 335) = 11.44,
p = .02, ε² = .03. Pairwise post-hoc tests indicated that the youngest age group “below 30 years” exhibited lower disapproval scores (Mdn = .75, MAD = 1.1) compared to the 40–49 years age group (Mdn = 5.51, MAD = 2.8), which showed the highest disapproval ratings,
p = .015 (see
Figure 5F). Despite these differences, an overall trend related to age was not observed, as Spearman's correlation revealed a nonsignificant relationship between participants’ age and their HAD scores,
r(333) = .05,
p = .396. Conversely, HAD scores did not significantly vary across musicians with different types of HL,
H(2, 335) = .44,
p = .8; see
Figure 5E.
Hearing aid Usage
The proportion of respondents using hearing aids was low. Only 7.8% of respondents (Ntotal = 31) reported using hearing aids or having tried them in the past. This usage rate was slightly lower among amateurs (6.5%, N = 13) compared to professionals (9%, N = 18). The average duration of hearing aid use among these individuals was approximately 9 years, with a slightly longer average usage reported among amateurs (9.8 years) versus professionals (8.6 years). Among those participants who reported wearing hearing aids, a large majority (79.7%) reported improvements in their hearing (“agree” or “totally agree”). However, the benefits from hearing aids appeared to be uneven across different auditory tasks. Those respondents who reported to use hearing aids regularly (Ntotal = 15) found hearing aids to be at least somewhat helpful for speech (100%). Similarly, 73% (N = 11) reported benefits for listening with ambient noise in the background. However, the effectiveness of hearing aids for music listening was deemed inadequate by many, with only 60% (N = 9) finding them useful for this purpose. This issue was further underscored by 54% (N = 8) of respondents who reported the quality of hearing aids as “rather not sufficient” for making music. Consequently, many refrained from using them, with 33% (N = 5) reporting they never used hearing aids for music listening.
Health-Related Quality of Life
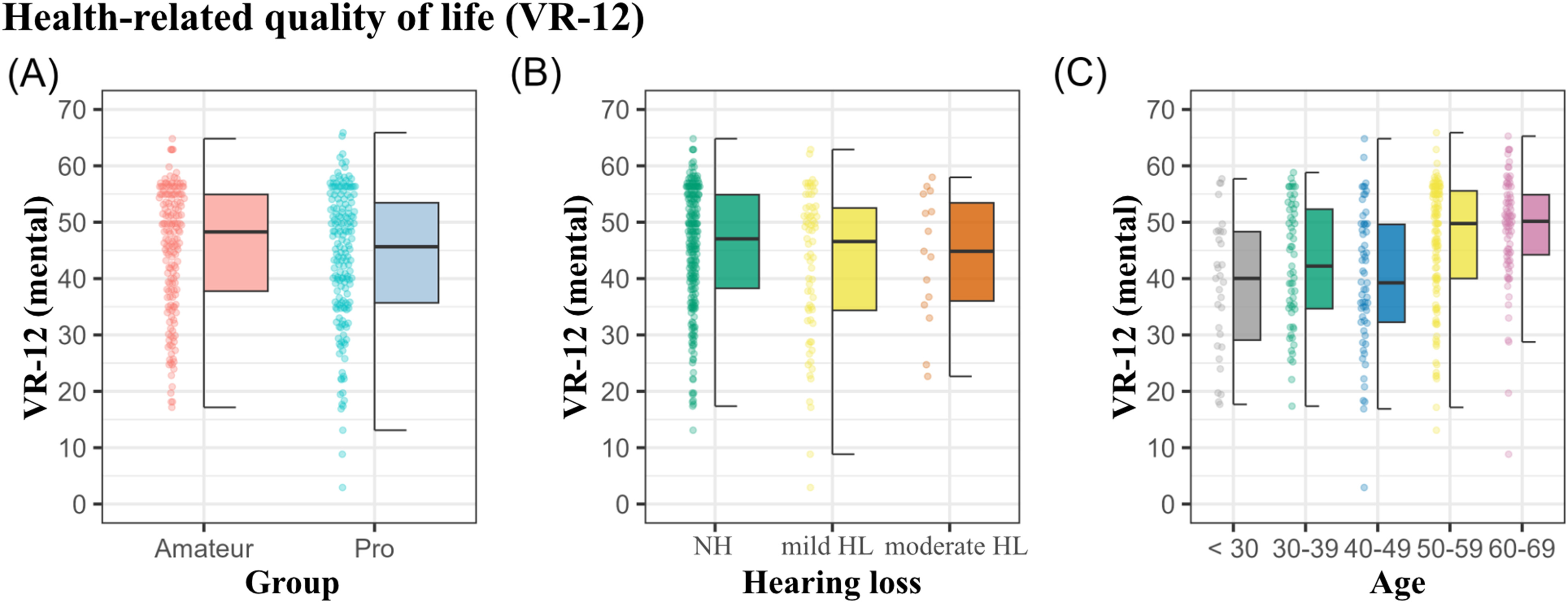
In the evaluation of veterans health-related quality of life scale (VR-12), no significant differences were observed between amateur and professional musicians with respect to the mental health component score, VR12-MCS;
W(353) = 16,465,
p = .35, see
Figure 6, or the physical health component score, VR12-PCS;
W(353) = 16,435,
p = .37. Furthermore, no differences could be observed between different degrees of HL and the VR-12,
H(4,364) = .58,
p = .75. However, the mental health component score correlated with age,
r(364) = .29,
p < .001, with musicians below 30 years reporting the worst mean scores (
M = 38.6, SD = 12), and the oldest age group of 60 + years the least inclination of mental quality of life issues (
M = 48.9, SD = 9.5).
Interscale Correlation Analysis
In the interscale correlation analysis, significant correlations among variables related to age, MRHPs, hearing in daily life, HHA, and health related quality of life indicators were found (for detailed correlation matrices, see
Table 2). Specifically, a positive relationship was found between the UNE and HHA,
r(330) = .24,
p < .001, indicating that individuals with higher noise exposure report greater awareness of hearing health related issues. Furthermore, a relationship was observed between HHA and the HDDA subscale for social interactions,
r(350) = −.32,
p < .001, and with MRHP,
r(345) = .20,
p < .001. Besides that, MRHP was moderately correlated with the HDDA subscale for social interactions,
r(365) = −.39,
p < .001. These findings imply that difficulties in hearing, both in social and musical contexts, often co-occur and are associated with heightened awareness of hearing health. Intriguingly, however, the UNE did not significantly correlate with either the HDDA subscale for social interactions,
r(355) = 0,
p = .75 or MRHP,
r(342) = −.08,
p = .152. Lastly, there was a notable negative correlation between MRHP and the mental health component of quality of life,
r = −.23,
p < .001.
Discussion
A focal point of this investigation was to determine whether professional musicians would (a) report a greater incidence of hearing problems and (b) exhibit a heightened awareness toward hearing health compared to their amateur counterparts. To allow for a nuanced comparative analysis between these musicians, a carefully curated and balanced subsample of 200 professional and 200 amateur musicians, matched based on age, gender, and instrument family parameters was established.
Noise Exposure and Musicians Hearing Problems
The comparative analysis highlighted notable discrepancies in weekly music exposure, with professionals averaging 30.9 hours and amateurs 7.4 hours of active playing. These figures align with prior findings, stating average practice times of 24–30 hours per week for professional musicians (e.g.,
Laitinen et al., 2003,
Schmidt et al., 2011). The study considered estimates of sound level exposure across various playing settings, from solitary practice to full orchestral rehearsals, alongside the attenuation of music noise exposure via hearing protection usage, thereby establishing a measure for lifetime music noise exposure. The results revealed that professional musicians experience almost three times the yearly music sound exposure and nearly four times the lifetime exposure compared to their amateur counterparts. This significant disparity persists despite a higher occasional usage of hearing protection among professionals (53.5%) compared to amateurs (12%). Examining lifetime exposure, 50% of professional musicians, as opposed to ∼10% of amateurs, reached an exposure level equivalent to experiencing 90 dB-A for 8 hours daily, 5 days a week, over 52 weeks annually, for a decade. Such levels of exposure, accumulated solely through music playing, are alarming, as they mirror conditions known to cause permanent HL, as documented in various studies and guidelines (e.g.,
Imam & Hannan, 2017;
Liedtke, 2010; see also “Königsteiner” and “NIOSH” recommendations;
Chan, 1998;
Deutsche Gesetzliche Unfallversicherung, 2013,
2020).
As a consequence of these high levels of music sound exposure, it was hypothesized that professional musicians would experience more severe hearing problems—both music-related and in daily life contexts—compared to amateurs. Indeed, two thirds of the musicians reported some kind of hearing problems. But despite the reported differences in musical engagement and its influence on music noise exposure levels, almost no group differences in reported hearing problems could be observed. Specifically, professional and amateur musicians reported comparable rates of self-reported HL (22% amateurs vs. 23% of professional), experiences with tinnitus (23.3% amateurs vs. 24.7% of professional), and oversensitivity to loud sound levels (44.8% amateurs vs. 53.3% of professional). Also scores from the MRHP scale and the subscore of the HDDA subscale for basic sounds did not differ significantly between professionals and amateurs. Furthermore, we could neither find an association of noise exposure with HDDA or MRHP, nor could we predict differences between the degree of HL with the music UNE. There was only one domain in which professional musicians reported significantly more severe hearing problems compared to amateurs: in the HDDA subscore for social interactions—with a rather small effect size.
The reported prevalence of hearing disorders among musicians, as found in this study, aligns with prior surveys (e.g.,
Harper, 2002;
Hasson et al., 2009), yet the lack of a significant difference between professional and amateur musicians in terms of hearing impairments, despite differing levels of music noise exposure, is notable. This observation resonates with challenges faced by other researchers, such as
Prendergast et al. (2017) and
Russo et al. (2013), who also reported difficulties in establishing a straightforward link between levels of noise exposure and hearing impairments among musicians (see also
Maghiar et al., 2023). Several reasons may account for these findings.
One possible explanation is that perceptual differences in hearing impairments that result from prolonged noise exposure may manifest gradually and too subtle for detection through self-report methods. Furthermore, musicianship has been linked to enhanced auditory abilities such as improved rhythm perception, pitch discrimination, and timbre identification (e.g.,
Grahn & Rowe, 2009;
Micheyl et al., 2006;
Nave-Blodgett et al., 2021;
Tużnik et al., 2018;
Zendel & Alain, 2012). There is even some evidence suggesting musical training may also benefit speech perception (
Coffey et al., 2017), which is, however, still under debate (e.g.,
Madsen et al., 2019;
McKay, 2021). Accordingly, musical training might be conceived to compensate for the negative effects of hearing impairments. Considering that two-thirds of the participants in this study are under 60 years of age, the subtle nature of noise-induced hearing changes, coupled with potential compensatory mechanisms developed through auditory training, could make early detection challenging. Thus, broad survey methods may not effectively capture these nuanced individual variations and contexts. Future studies should consider integrating hearing assessment methods, such as high-frequency extended pure-tone audiometry (e.g.,
Couth et al. 2020,
2024), to validate self-reported data and ensure more robust findings.
Another potential explanation of these findings could relate to the operationalization of the unit of UNE score. This metric, designed to provide a coarse estimate of prolonged noise exposure, is based on several assumptions that may affect its precision in identifying correlations with hearing problems. A key factor is the specific instrument and the repertoire played by musicians, as these can significantly impact sound exposure. For example,
Schmidt et al. (2011) noted a substantial difference of 9.6 dB between repertoires, underscoring the repertoire as a significant factor in musicians’ exposure (also see
Laitinen et al., 2003;
Rodrigues et al., 2014). Moreover, the model adopts a conservative approach, considering a constant noise exposure during individual practice from the age of 10 and orchestral/rehearsal noise exposure from age 20. This cross-sectional method does not account for variations in playing times throughout a musician’s career and life, instead it presumes a constant exposure over time. Furthermore, the NESI examination instrument (
Guest et al., 2018) used to calculate the musicians’ sound level exposure was originally designed to capture both occupational and recreational activities. However, in this study, it was only applied to sound exposure from instrumental music encountered during active music-making activities. Recreational music listening and other everyday sources of noise exposure were not considered.
Couth et al. (2020) utilized the same instrument but included recreational activities to calculate the total lifetime noise exposure between musicians and nonmusicians (not specifically excluding amateur musicians), finding similar levels of exposure for both groups when recreational activities were included, as the majority of noise exposure could be attributed to recreational activities. Accordingly, in our sample, the musicians’ total lifetime noise exposure may be more similar when recreational activities are taken into account, which could explain the lack of differences in reported hearing problems between professional and amateur musicians. It is conceivable that employing more detailed estimates, which account for different career phases and other noise exposure contexts, might uncover effects that the current methodology does not detect. Still, recent work by
Couth et al. (2024) also shows minimal effects on hearing from noise exposure utilizing a longitudinal design, suggesting that the effects observed in this study may remain stable over time.
Certainly, establishing a direct link between musical sound exposure and hearing impairments proves challenging (see also
Couth et al., 2020;
Elmazoska et al., 2024;
Kähäri et al., 2001a;
2001b), which suggests that the risk of noise-induced HL in musicians might have been overestimated in previous research. Additionally, there is evidence that occupational noise, such as that encountered on construction sites, may be more detrimental to hearing than recreational sound, including music, possibly due to the dynamic nature of musical sounds (
Neitzel & Fligor, 2019). Nonetheless, it is crucial to recognize that many musicians, both amateurs and professionals, are exposed to exceptionally high noise levels during their practice and performances. This exposure is particularly pronounced during individual practice sessions, where long uninterrupted playing and infrequent use of hearing protection are common. Thus, in sum, these findings underscore the importance of preventive measures to preserve musicians’ hearing health.
Preventive Measures and Hearing Health Awareness
While hearing protection devices offer great potential for improving musicians’ hearing health, their utilization remains alarmingly low. The analysis showed greater (occasional) usage of hearing protection among professional musicians (53.5%) compared to amateurs (12%). This is evident despite 73% of professionals reporting that hearing protection impedes their performance; yet, musicians continue its usage, demonstrating a complex balance between auditory health and musical quality. The majority of musicians who use hearing protection opt for customized solutions (professionals: 84%; amateurs: 65%), indicating an understanding of the importance of personalized fit and comfort. However, a concerningly low 1% of amateur musicians’ playing hours and only 9% of professional musicians’ playing hours are fully protected. In contrast, 80% of amateurs’ and 36% of professionals’ playing hours remain completely unprotected. Given the potential benefits of hearing protection (e.g.,
Kwak & Han, 2021), these numbers underscore the need for action to promote greater hearing protection adoption within the music community. Intriguingly, musicians demonstrate a pattern of increasing HHA as their hearing problems worsen (as also noted by
Laitinen, 2005). This negative relationship exists in both music-related settings and social interactions and is mirrored in hearing protection usage: only 3% of those with NH use full protection, increasing to 5% for those with mild HL and a notable 22% for those with at least moderate HL. These findings support the “reactive action” phenomenon, where proactive measures are often taken only after issues arise.
The low utilization rate of hearing protection resonates with findings from nearly two decades ago, as reported by
Laitinen (2005), where 6% of Finnish musicians were noted to always use hearing protection devices. The stagnation in the adoption of protective measures, even considering variations among different countries, underscores the necessity for effective strategies and interventions that are specifically tailored to the unique needs of the music community. Several factors influence the notably low uptake of hearing protection across the musician community. On the one hand, legislative measures play a crucial role; an overwhelming majority of professionals (97%) regularly undergo hearing checks, typically every three years, as contrasted with 70% of amateurs, who tend to seek audiologist consultations only once every seven years on average. Accordingly, such regulatory mandates, as outlined in the German
Noise and Vibrations—Occupational Safety and Health Ordinance (2007), are likely central in promoting higher rates of hearing protection use among professional musicians. Performance-related anxieties, on the other hand, contribute to the reluctance in adopting hearing protection; 80% of professionals and 32% of amateurs who refrained from using hearing protection said they refrained from using hearing protection because they are concerned their performance might suffer. However, the primary factor is the lack of awareness about hearing health issues. On average, amateur musicians exhibited considerably lower average awareness scores compared to professional musicians. This discrepancy is most evident among younger musicians who, despite facing higher music noise exposure, are least inclined to use hearing protection. This finding contrasts with the report by
Couth et al. (2021), which indicated that 77% of young musicians employ hearing protection at least once a week. Intriguingly, young musicians (<30 years) in this study had the highest awareness scores, prompting a re-evaluation of the direct association between awareness and behavioral change as proposed by
Ajzen (1991) and underscores the complexity of translating awareness into action.
In conclusion, while establishing a clear link between heightened awareness of hearing health and the consistent use of hearing protection proves challenging, expanding regulatory measures to encompass amateur orchestras could offer substantial benefits. Furthermore, addressing performance-related anxieties and providing information on adaptation processes to mitigate performance impacts could be pivotal components of awareness programs (see also
Couth et al., 2021 for model strategies).
Hearing aid Usage
A mere fraction of musicians across both professional and amateur settings (N = 15) reported continuing usage of hearing aids, highlighting a noteworthy yet anticipated low utilization rate. Furthermore, 54% of these users expressed that their hearing aids are not sufficient for making music, and only 80% reported that hearing aids improve their hearing at all. This finding aligns with existing literature indicating that current hearing aid technologies may not sufficiently cater to the specialized auditory needs of musicians: Previous survey studies have demonstrated that although hearing aids were perceived as useful in listening to both live and recorded music, their efficacy was deemed less satisfactory for live musical settings—a context of paramount importance for musicians. Common issues reported include distortion, acoustic feedback, imbalanced gain, and compromised tone quality (
Madsen & Moore, 2014). However, it is essential to acknowledge more recent studies presenting a more favorable view. These suggest that hearing aid usage can indeed improve music enjoyment and appreciation for both speech and music (
Chern et al., 2023).
One major concern in this research centers on the potential underrepresentation of individuals with severe hearing impairments who have found hearing aids to be ineffective for musical tasks. Such individuals may have withdrawn from musical activities altogether, thereby becoming statistically invisible within the current study sample. Indeed, more than half of the respondents who reported having tried hearing aids in the past (16 out of 31) refrained from using them. This phenomenon may correspond to an instance of “survivorship bias,” an analytical error characterized by an undue focus on subjects that “survive” a given process while overlooking those who do not. Those subjects who report finding hearing aids effective are likely those who have persisted in musical activities despite hearing challenges. This could inadvertently exclude the experiences of those who have ceased musical involvement due to the inadequacy of hearing aids for music-related tasks. The recognition of survivorship bias and its potential impact on the study’s findings has significant implications for this research's validity (that is, the reported utility rating are likely an overestimation of the usefulness of hearing aids), but also has implications for future investigative directions: Subsequent studies could adopt sampling techniques specifically designed to capture the experiences of individuals who have withdrawn from musical activities due to the limitations of hearing aids and hearing impairments. By doing so, a more comprehensive and accurate understanding of the true effectiveness and limitations of hearing aids may be attained, especially in the domain of music perception and performance.
Our findings further underscore the pivotal role of attitudes toward hearing aids as a moderator in the adoption and sustained utilization of hearing aids among musicians. In our study, professional musicians manifested a markedly higher degree of disapproval toward HAD compared to their amateur counterparts. Moreover, one out of four musicians indicated hesitancy in openly discussing their HL in public. This differential disapproval may be anchored in both the stigmatization of hearing aids and their perceived functional limitations within professional musical settings. The constructed scale for HAD encapsulates multiple facets that resonate with this notion, including irritation caused by colleagues wearing hearing aids, reluctance toward nondiscrete devices, apprehensions about diminished peer respect, adverse audience perceptions, and the presumed incongruence between professional musicianship and hearing aid use. These elements collectively converge to form a pervasive stigma surrounding hearing aids, particularly within the realm of professional musicianship. The implications of this aversion are twofold. First, it elucidates an unexplored barrier to hearing aid adoption among a specialized population. Second, it offers a fertile ground for targeted interventions designed to mitigate these attitudes, thereby potentially augmenting hearing aid uptake and sustained usage among professional musicians. Additional empirical inquiries are imperative for a conclusive understanding of the dimensions and implications of hearing aid aversion in this particular cohort.
Importantly, the distribution of HAD among musicians presents a bimodal pattern. While a considerable majority exhibits minimal disapproval, a notable subgroup demonstrates substantial disapproval of hearing aids. There is some indication that older individuals tend to express higher disapproval toward hearing aids, yet a straightforward relationship could not be observed. Certainly, age-dependent inclination toward hearing aid aversion merits further empirical scrutiny, as it could have broader implications for targeted interventions aimed at enhancing hearing aid adoption among ageing musicians.
Musicians’ Overall Well-Being
No differences in terms of the health-related quality of life scale could be observed between professional and amateur musicians. The overall state of both physical and mental health in our sample of amateur and professional musicians can be characterized as healthy. This claim is substantiated when comparing published benchmark values from populations undergoing healthcare challenges. For instance,
Buchholz et al. (2017) reported mean scores of 33 on the physical sum scale and 41 on the mental sum scale in a population of patients undergoing orthopedic rehabilitation. Similarly, a study by
Hüppe et al. (2022) involving patients with chronic pain reflected comparable results with average scores of 28.1 and 37.6 on the physical and mental scales respectively. In comparison, musicians from this study’s sample demonstrates a substantially healthier profile, which aligns more closely with scores anticipated from a generally healthy population. However, there is considerable variability in the subscale for mental health among participants, with 113 musicians scoring below 40 (comparable to orthopedic rehabilitation; see
Buchholz et al., 2017) and 48 scoring below 30 (comparable to chronic pain; see
Hüppe et al., 2022). Notably, a significant proportion of those with lower scores are in the youngest age group, indicating that younger individuals tend to have poorer scores on mental health. This is consistent with previous research into musicians’ psychological well-being; for example,
Kenny et al. (2014) found that the youngest (female) musicians often report the highest levels of performance-related anxiety. Despite this, an increase in hearing issues related to music and in daily-life was associated with a decline in mental health-related quality of life, suggesting a significant psychological toll from these impairments.
Limitations
Several limitations must be acknowledged to contextualize the present findings. First, despite the efficacy of the matching procedure in equalizing pivotal variables such as age, gender, and instrument type, additional imbalances—such as the differences in repertoire played—could not be completely controlled for. Second, the process of matching inevitably led to the exclusion of certain participants, thus reducing the sample size. Nevertheless, the remaining sample (N = 400) was sufficiently robust to yield statistically meaningful insights. Importantly, the matching strategy served to better isolate the effects of the variables of interest by minimizing potential bias due to confounding variables, thereby justifying the concomitant reduction in statistical power.
A potential self-selection bias poses a concern for the generalizability of the results. The voluntary nature of participation suggests that the sample might disproportionately represent musicians with a particular interest in hearing health, possibly due to personal experiences with hearing impairments. Consequently, the findings may exhibit a bias toward greater HHA, or a higher incidence of hearing issues compared to the general population of musicians, thereby limiting the generalizability of the results. However, it should be noted that many of the findings align with prior research on hearing health among musicians, not just in Germany but also in countries such as Australia and Finland, yielding corroborative evidence to the present study.
Additionally, the study’s reliance on self-reported data introduces another layer of complexity. For example, existing literature suggests that participants in survey research often overstate socially desirable behaviors (e.g.,
Tourangeau & Yan, 2007), thereby introducing measurement error. This remains uncontrolled and might induce bias, particularly among musicians who are acutely aware of their auditory capabilities and may report subtle issues irrespective of actual noise exposure. Nevertheless, this propensity for “over-reporting” is more pronounced in interviewer-administered surveys than in self-administered questionnaires, especially when the latter are conducted anonymously and voluntarily. Hence, while the present study has attempted to mitigate this bias through its design, the possibility of misrepresentation of certain attitudes still warrants cautious interpretation of the findings.