Background
Heart failure (HF) is the common endpoint of multiple cardiovascular diseases and remains a leading cause of mortality and morbidity worldwide.
1 It is characterised by progressive symptom burden, frequent hospitalisations, and substantial impact on quality of life.
2 Beyond physical symptoms, HF also imposes significant psychological and social challenges for both patients and their caregivers, particularly in the advanced stages of illness.
3Patient education and supportive coaching programmes are increasingly recognised as integral to holistic chronic disease management. One such programme is Educate, Nurture, Advise, Before Life Ends (ENABLE), originally developed for patients with advanced cancer in the United States. ENABLE provides guidance on symptom self-management, psychoeducation on coping strategies, and steps for future care planning.
4,5 Given its positive impact on patient outcomes, ENABLE has been adapted for other populations, including those with HF.
4,5A feasibility pilot of ENABLE Comprehensive Heartcare for Patients and Caregivers (ENABLE-CHF-PC) demonstrated moderate improvements in patient quality of life, symptom burden, and mental and physical health, as well as caregiver quality of life, mood, and burden. Modest reductions in hospital and intensive care unit (ICU) length of stay were also observed.
6 While the larger randomised controlled trial failed to show a significant benefit in primary outcomes (quality of life and mood), it yielded clinically significant reductions in pain intensity and interference.
7To date, existing trials have primarily focused on clinical endpoints and patient-reported outcomes, without adequately assessing whether interventions meet patient expectations or address their lived needs. This gap in understanding constrains the refinement of supportive interventions and risks overlooking the very perspectives that determine their acceptability and impact in practice.
Building on this evidence, our study team adapted the ENABLE-CHF-PC programme for the Asian care context in Singapore and evaluated its impact on patient and caregiver outcomes through a wait-list randomised controlled trial.
8 In this paper, we focus on the experiences of participants as they pertain to their illness journeys and to the programme: how they navigate HF, the ways in which health coaching addressed their needs, and the areas in which expectations or needs remained unmet. While our findings are situated in the ENABLE framework, they offer insights that are broadly applicable to the design and delivery of health coaching and patient education interventions for the HF population.
Methods
Study design and setting
This qualitative study involved conducting in-depth individual or dyadic semi-structured interviews with a sample of patients and caregivers who completed the ENABLE programme delivered at the National Heart Centre Singapore (NHCS). NHCS is a national and regional referral centre for cardiovascular diseases in Singapore that manages more than 140,000 outpatient consultations and 10,000 inpatients each year.
9 This study formed part of the ENABLE Intervention for Heart Failure Patients and their Caregivers in Singapore (ENABLE-HF-SG) trial, registered on ClinicalTrials.gov (ID: NCT05211882).
8Ethical issues
This study obtained approval from the institutional review board at the SingHealth Centralised Institutional Review Board (CIRB), reference number: 2021-2722, and was conducted in compliance with the Declaration of Helsinki.
Written informed consent for participation in the parent ENABLE-HF-SG trial included agreement to be contacted for a post-programme interview. At the time of the interview, participants also provided verbal consent to proceed. Risks to participants were minimal. All data were de-identified prior to analysis and stored on secure devices. Access to data was restricted to authorised study team members. Although no participants experienced distress during interviews, procedures were in place to allow participants to pause or stop the interview, with referral pathways to psychosocial support available if needed.
Inclusion and exclusion criteria
All participants were 21 years old and above and English or Mandarin-speaking. Patients had to be diagnosed with stage C or D HF by the American College of Cardiology guidelines, of New York Heart Association (NYHA) functional class II, III, IV, on disease-directed HF management, deemed to have a prognosis of at least 6 months based on clinical notes and/ or clinician assessment, and have a hospitalisation episode in the 6 months prior to recruitment. Patients did not have prior contact with specialist palliative care services. Caregivers were direct family members of the patient. Patients and caregivers did not have to participate in the interviews as a dyad.
Purposive sampling ensured diversity in age, HF severity, and study arm. Participants were invited by telephone by the study research coordinator to share their programme experience in an interview. Although 10 female patient participants completed the intervention, none agreed to participate in post-intervention qualitative interviews. Recruitment proceeded until no new codes emerged in three consecutive interviews.
10 The sample size was consistent with recommendations for thematic analysis
11 and prior qualitative studies in advanced HF populations.
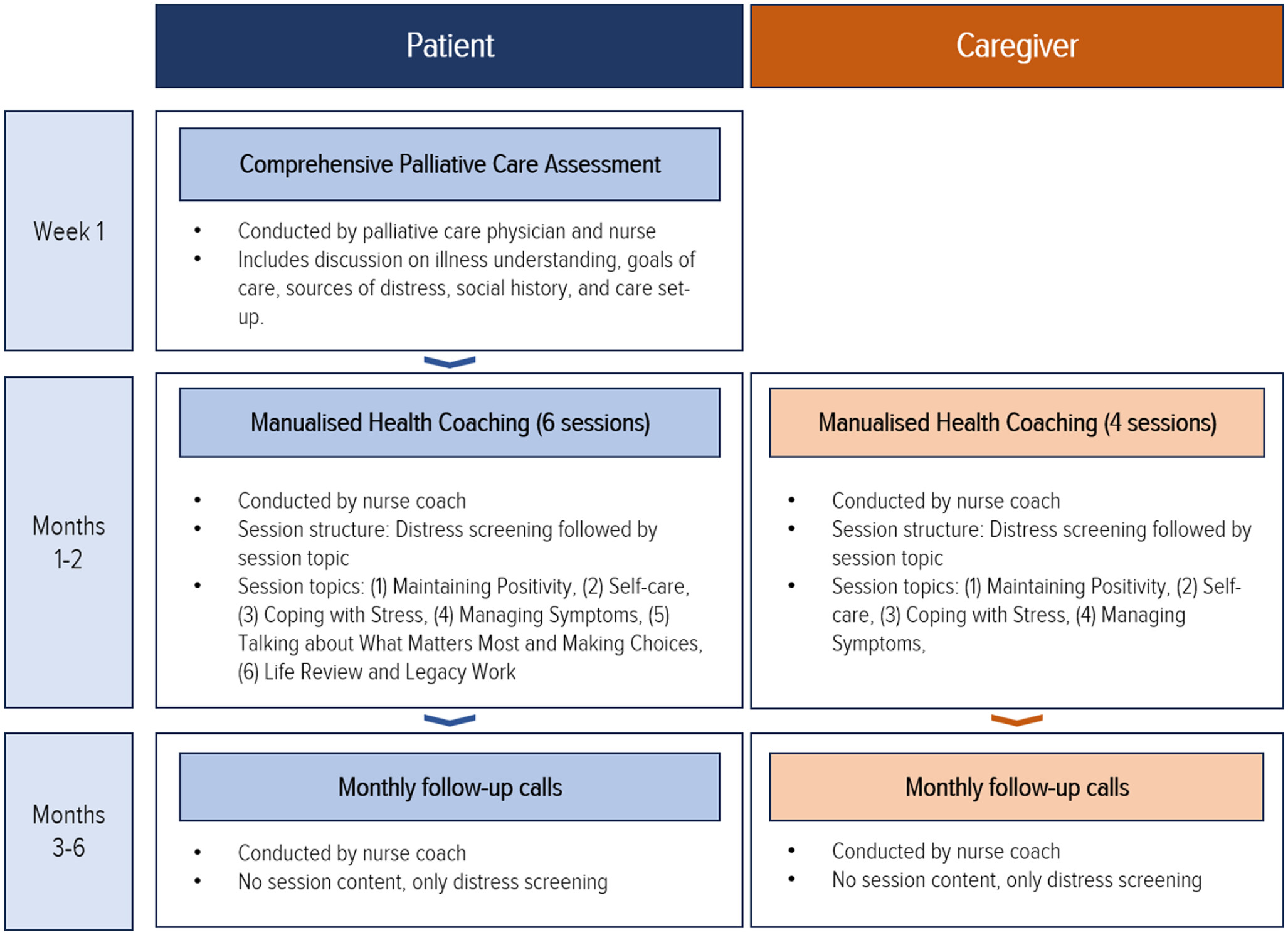
12–14Details of the culturally adapted ENABLE programme
The ENABLE programme involved three separate components: a comprehensive palliative care assessment, a manualised health coaching curriculum (Charting your Course), and follow-up phone calls (
Figure 1). Sessions were delivered in person or via secure video-conferencing, either individually or as patient-caregiver dyads.
Data collection and analysis
Data collection took place from March 2022 to March 2024. We adopted an interpretive phenomenological orientation, aiming to understand how patients and caregivers made sense of living with HF and participating in the ENABLE-CHF-PC programme. This orientation helped elicit rich accounts of lived experiences while allowing participants’ perspectives to guide the analytic focus. An interview guide was used to explore participant experiences (
Supplemental Appendix 1). Interviews were conducted via telephone by a full-time research coordinator not involved in recruitment or intervention delivery, and who had no prior relationship with participants. Interviews lasted between 30 and 60 min, were audio-recorded with permission, de-identified, and transcribed verbatim.
We conducted a reflexive thematic analysis following Braun and Clarke.
15,16 Two coders (Y.S., A.N.) independently read the transcripts for familiarisation, generated initial codes, and developed a preliminary coding framework on Microsoft Excel. Although both coders were unfamiliar with ENABLE-CHF-PC, Y.S. had 3 years of health coaching experience in chronic disease and cancer care, and A.N. had prior exposure to HF management through palliative care research at NHCS. These backgrounds inevitably shaped their preliminary interpretations of participants’ accounts. Both researchers engaged in regular team discussions to examine how their assumptions and experiences influenced coding and theme development.
Following multiple discussions to resolve coding discrepancies, Y.S. and A.N. refined candidate themes to produce the final analytic themes. To enhance trustworthiness, we maintained an audit trail using analytic memos and engaged in regular debriefs. Reporting follows the Standards for Reporting Qualitative Research (SRQR) guidelines (
Supplemental Appendix 2).
17Demographic information was also obtained from participants at baseline when they enrolled in the wait-list controlled trial. While no quantitative data were collected specifically for this qualitative component, these demographic variables were used descriptively to contextualise the interview sample.
Results
We recruited 14 participants (8 patients, 6 caregivers) who completed the ENABLE-CHF-PC coaching programme for this study. Demographic characteristics of the 14 participants are presented in
Table 1. All patient participants were male and most caregivers were female, with most identifying as Chinese. These characteristics reflect the demographic profile of the HF population and their caregivers typically seen at NHCS.
Three themes were generated from our data (
Figure 2).
Theme 1: Participants need orientation to manage HF
Many patients described feeling lost and uncertain about how they can manage their HF and live meaningfully with it. Two main factors, unmet information needs and uncertainties about how to move on with life, contributed to this sense of disorientation. Without support, patients were unsure of how to navigate physical and emotional symptoms. Consequently, some adopted counter-productive self-management strategies, while others struggled with the loss of meaningful or personally satisfying activities in their lives.
Disorientation due to unmet informational needs
Patients reported having many unanswered questions about their condition. This was attributed to a few factors. First, follow-up appointments were infrequent, with relatively asymptomatic patients seeing their cardiologists only once every 6–8 months. Informational support between consultations, according to some, seemed inaccessible.
Along the way, I find something not good or I find the medicine not really. . . or I feel something wrong with the medicine, I want to check, I don’t know who to ask also. It’s very difficult for you to find back the doctor also. (Patient (Pt) 04, Male, 46)
Secondly, even during follow-up appointments, patients struggled to get the clarity they desired. Some patients perceived that there was insufficient time to ask all their questions and receive comprehensive answers during their consults. Another patient commented that he would prefer having more context and information than what was offered by his cardiologists: “I think for my condition right, it is one of those, you don’t take [the medication], you die. So [the doctors think that there is] no need to talk about side effects, just take. You know, but at least let me know.” (Pt13, Male, 43)
Finally, these unanswered queries could also be attributed to patients not reaching out to available supportive services. While NHCS offers a HF hotline, many participants did not use it, either out of a concern that the hotline is too “serious” (Pt57, Male, 47) for their issues or a preference to have direct access to their doctors:
Whether it’s a heart failure hotline or what, you can’t contact the doctor. You only can contact the nurse[. . .] What if you need immediate answer from the doctor which the nurse can’t answer? (Pt18, Male, 50)
These informational gaps, compounded by the perceived inaccessibility of medical expertise, heightened anxiety and uncertainty in participants.
Because not knowing any symptom or any problem with yourself or your current situation, it can be a bit . . . worrying . . . I don’t know what’s happening with me, you know. (Pt05, Male, 32)
In the absence of clear medical guidance, some adopted unhelpful practices, such as overly restrictive diets.
A lot of thing(s), you (are) scared, I don’t know what to touch also. At night I eat with my family, I don’t take rice, anything. I only eat some of the dish, then I eat a lot of fruits. (Pt04, Male, 46)
On occasion, these misinformed practices could even be dangerous. For instance, a caregiver described her initial uncertainty about how to respond to the patient’s frequent urination. She only realised the need to seek medical attention upon consulting the nurse coach. Without access to the nurse coach, the patient would likely have just “ke(pt) on (staying) at home alone, ke(pt) on passing the urine” (Caregiver (Cg)18, Female, 78). This underscores the importance of orienting patients and caregivers to the patients’ condition by providing a comprehensive informational scaffold of HF symptoms and management strategies.
Disorientation due to uncertainties about how to move on with life
Participants reported facing difficulties moving forward and living meaningfully with their condition. Many found themselves struggling with the loss of activities they had previously enjoyed.
Participants characterised HF as a restrictive condition, with compliance to medical recommendations necessitating the discontinuation of activities that brought them joy and satisfaction. Adapting to living with HF meant displacing the very pursuits that often enhanced their emotional well-being.
You see there are certain things, at this point of my life, I’m given a lot of medication, a lot of restrictions on water, restrictions on food, and so on. [. . .] Sometimes a person we need food just to keep you happy. (Pt36, Male, 74)
Often, these changes involved abstaining from travel or physical activity. While these activities were not necessarily harmful, patients reported feeling fearful about the risk of aggravating their condition or facing a medical emergency when engaging in these activities.
For me, only future worry is that I want to travel. Eventually I want to go see the world and just enjoy life. But at the same time, of course, this will be at the back of my mind la. [. . .] If I go overseas and the hospitals are 2, 3 hours away, you don’t know what to anticipate. (Pt05, Male, 32)
Aside from having to navigate the loss of meaningful activities, living with HF also affected the patients’ outlook on life, with many describing a nagging worry of mortality.
Because once you have the heart attack, you start thinking about—besides thinking about your health—you think about what will happen if I go. . . . So, even now that I’m doing better, I also think of. . . there’s this thing at the back of my mind, it’s like: how long will I last? You know, am I a ticking time bomb? (Pt12, Male, 61)
While such uncertainties motivated planning for end-of-life care in some, they fuelled anxiety about having goals-of-care discussions in others.
Because I find it very difficult to talk to [Pt17] about the next step, about DNR [Do Not Resuscitate]. [. . .] She will keep quiet, she’ll keep it in her head. And then eventually it comes out in (the) form of. . . anxiety, the fear. (Cg17, Male, 65)
With a return to their pre-illness “normal” foreclosed, participants highlighted a need for guidance in making lifestyle adjustments and coping with health-related anxieties. Consequently, patients find that they are unable to “go back to their normal lifestyle before the whole thing happened” (Pt04), and must instead find ways of living meaningfully with the restrictions and uncertainty of their condition. Given the difficulty of this task, many patients (and in some cases, their caregivers) needed support to make the requisite lifestyle adjustments and to cope with difficult emotions attendant to the magnitude of change they faced.
Theme 2: Health coaching orientates participants by enhancing their sense of control and security
Participants identified two main benefits to health coaching: (i) gaining personalised information and (ii) having a direct line of access to a nurse coach. Personalised information, as compared to structured programme materials, bolstered the participants’ confidence in managing their condition and engaging their clinicians. Meanwhile, having access to a nurse coach who was perceived to be experienced and knowledgeable helped patients to find a source of security as they lived with the uncertainties of HF.
Personalised information increased participants’ sense of control
Participants valued gaining a “better insight and a better understanding of what [the patient’s] condition is” (Pt05). They indicated a preference for condition-specific information about medication side effects, symptom management, and when they should seek medical care. Having such information enhanced the participants’ sense of control in managing their condition and their confidence to engage more proactively with their cardiologists.
Then she [nurse coach] tell me what drugs have what side effects, then roughly I know, “Oh, this is not me going crazy, (it) is the drugs making me go crazy.” Because . . . when I first started taking all the pills, I had to go to the toilet once every 15 minutes. [. . .] (So) I asked the doctor, “Is there any pill here that gives me super pee or not?” Then he said, “Yeah, I mean this one makes you pee non-stop. Actually it’s optional.” Walao eh! [slang for exclamatory “what!”] . . . I say, “I don’t have problems peeing, I don’t need that pill.” (Pt13, Male, 43)
The informational support provided by the nurse coach also helps caregivers feel more equipped at supporting their loved ones.
Then at least I can tell him to do things. Otherwise, (for) heart failure, you don’t know whether to tell him to exercise or not, tell him to walk or not. (Cg18, Female, 78)
In contrast, responses to the structured ENABLE guidebook were mixed. While some appreciated its comprehensiveness or addressing of topics like self-care (Cg13, Female, 42) and “keeping memories” (Pt57, Male, 47), most struggled to recall or apply its content.
What 6 topics? [. . .] I don’t remember, seriously. You say 6 topics, guidebook, all these things. No impression ah. (Pt13, Male, 43)
In some cases, participants also found the content irrelevant or inappropriate.
I’m not the kind who also go for sexuality because . . . this is not the main thing in life, right? We have so many other important things in life. (Cg36, Female, 73)
Structured content on advance care planning and legacy work, in particular, provoked anxieties in several participants and was perceived to conflict with their desire to live and belief that they are “recovering” (Pt12, Male, 61)
To me, you hear already, it’s a bit 怕怕 (scary), but I find that every day I (am) ok la [a colloquial particle used for emphasis], healthy la . . . it’s good to plan for this—all this “last road” one—but very funny at the moment la. (Pt04, Male, 46)
In summary, the utility of the structured materials appeared limited insofar as they were of varying relevance to different participants. That the structured content was designed to be comprehensive may unexpectedly contribute to mixed results, as certain elements within evoked anxieties or hit an emotional nerve with some participants. This highlighted the value and importance of tailoring information to individual readiness, preferences, and needs, a sentiment echoed by some.
Maybe some topics. . . you put as optional and then you let them choose whether they want to do it or not. (Pt57, Male, 47)
Access to an experienced nurse coach increased participants’ sense of security
Participants emphasised the accessibility of support as critical to their sense of security. For many, the presence of a dedicated point of contact mitigated the anxiety associated with managing a chronic condition. As one participant noted, the ability to consult the coach allowed for a preliminary clarification of symptoms, reducing the cognitive burden of trying to understand “what’s wrong” on his own:
Every time I got a problem, I go look for (the nurse coach) and she’ll tell me what’s wrong, roughly. (Pt13, Male, 43)
This perceived availability of support translated into a broader sense of assurance and a source of security.
I feel more of a sense of security in that I can ask questions. (Pt57, Male, 47)
The sense of security described by participants extended beyond the perceived availability of help. Rather, it also stemmed from the perception that the nurses were credible clinicians and communicators who could translate otherwise complex medical information into “layman” terms (Pt57, Male, 47).
Whatever information she gives, she knows what she’s talking about. . . So it makes you feel comfortable. (Pt12, Male, 61)
Further, the nurse coaches’ willingness to accommodate the participants’ schedules and provide support at a level beyond what was perceived to be the scope of the programme demonstrated an ethic of patient-centred care that deepened the participants’ trust in their coaches:
Usually, I think she’s (working from) 8 to 5, but because of my schedule, she’s okay to do the [coaching] on the weekend. [. . .] Also, some of the questions I asked her, where should I get financial help from who or how to do this? She actually gave me some advice on it. (Cg43, Male, 57)
For certain participants distressed by their condition, the coach was seen as a source of emotional comfort or, as one caregiver described, “the light” during periods of feeling down:
During this time when we are so depressed and don’t know what to do, she could help me in every way, giving examples and kind of consoling and be the light. . .. (Cg36, Female, 73)
The rapport, frequently described in familial terms, suggested that the “genuine concern” exhibited by the coaches transformed the professional relationship into one of deeper personal significance:
We have built such a rapport with [nurse coach]—she’s so good, so concerned, you know, it’s genuine concern, and then, it becomes like friends, like big sister. (Cg05, Female, 64)
For both patients and caregivers, the quality of care evinced in the various abovementioned factors cultivated a sense of being cared for, alleviating the isolation often felt by participants in living with HF and contributing to a sense of security as they navigated the uncertainties and challenges of chronic illness.
It’s good that I feel that somebody is actually out there concerned in the sense. (Pt43, Male, 46)
Theme 3: Participants desired further support in helping them navigate the tensions of living with a life-limiting illness
Despite the perceived utility of the programme, participants highlighted a need for more practical, action-oriented guidance to support their goals of health improvement. Patients articulated that the provision of tangible, actionable information was a prerequisite for developing the self-efficacy necessary to manage their condition, while caregivers expressed a distinct desire for instrumental support to achieve technical mastery in specific caregiving tasks. Beyond the need for practical guidance, some participants exhibited difficulties living in the present and engaging in future planning, highlighting a need for complementary psychosocial support.
Desire for actionable information
Given the prevailing desire to adapt to their circumstances and lead a “normal life,” participants identified various gaps in the coaching programme. Most suggestions raised by participants centred on receiving more tangible and actionable guidance to improve their health. For instance, one participant reported that he needed more specifics to gain confidence in resuming physical activity:
The thing is. . . the person [doctor] never covered on how intense your exercise (can be) [. . .] How (about) a suggested [exercise] duration? Maybe 60 minutes, 70 minutes? There’s a number, a guideline for us. And what are the things you should avoid? [. . .] maybe wear a Fitbit watch, then you can monitor the heartbeat, not to go more than 120. (Pt57, Male, 47)
Another felt that the programme had “enriched [him] with good information that [he] can use” (Pt05, Male, 32), but pointed out that it failed to provide practical tips on how to sustain these lifestyle changes.
Caregivers also expressed a similar interest in tangible caregiving skills, like providing for the patient’s daily care needs and guidance on facilitating goals-of-care discussions with family members. “(The programme) is not so much on (physical caregiving) . . . to learn how to take care, you know. Actually, I don’t know how to take care.” (Cg43, Male, 57)
Need for psychosocial support
For some, adjusting to a new illness reality appeared to require additional psychosocial support, as their worries and concerns were not adequately addressed through patient education or coach-delivered informational support. For instance, despite having been cleared for air travel by his cardiologist, Pt04 reported feeling ill at ease about the idea. Living with the uncertainties of HF appeared to have cast a shadow over his life, even as he acknowledged his doctors’ advice.
I have this phobia. Now I go on top of aeroplane, and then what happen? [. . .] [Doctors] say go ahead [and travel]. Because everything checked, “your heart okay.” My heart (went) back to I think 70% already. [. . .] They tell you already, but 因为那个阴影 [there is still a shadow]. (Pt04, Male, 46)
More broadly, living with HF entailed grappling with the tensions of a dual consciousness: being aware of one’s illness yet feeling well; recognising the threat of sudden cardiac death or acute deterioration while striving for recovery and maintaining the hope of preserving a sense of normalcy.
I know heart failure is coming. I don’t know when it will come. I work out whatever I can, because the things do whatever (they do), I can eat whatever I can, and overall be as happy as I can (be). (Pt36, Male, 74)
Some sought to resolve this tension by relegating all discussions of illness, decline, and death to the background, describing such topics as “negative” or “
suay” (bad luck). Preferring instead to “maintain positivity,” they were sceptical about the value of reconstructing and making sense of their illness journeys:
The life story to me is not so relevant, because why (do) you want to know about your life story? [. . .] Not the past, you want the future. (Pt18, Male, 50)
Accordingly, coaching topics that touched on end-of-life care and legacy planning were deemed irrelevant and only appropriate in the patient’s final days.
You know, maybe you can approach it when the person is in (their) death-bed and all that, you know. So, you ask, have you signed your will? (Pt12, Male, 61)
However misaligned with the practical realities and goals of early legacy planning and goals-of-care discussion, these views underscored the ongoing existential challenge of living with this dual consciousness. This underscores the importance of support to reconcile one’s hopes for the future with the ever-present threat of illness and death.
Discussion
This study explored the needs of patients with HF in Singapore, with the aim of understanding how the intervention benefited patients and identifying persisting needs that the intervention was unable to meet. Across the three themes, participants described the disorientation that accompanied an HF diagnosis and the challenges of navigating their condition while striving to rebuild or maintain a sense of normalcy in daily life. Health coaching mitigated these challenges by providing personalised and accessible professional support, which enhanced the participants’ sense of control and security. However, participants’ responses pointed to outstanding informational gaps, health-related anxieties, and an overarching existential ambivalence. These findings suggest that supporting patients with HF requires not only information and skills training, but also individualised and integrated psychosocial support that addresses a complex assemblage of informational, emotional, and existential needs.
The needs identified in this study are consistent with and enrich findings from existing literature on the experiences of patients with HF. Existing research highlights how the illness is experienced as disruptive, requiring major lifestyle adjustments and having a significant emotional impact on patients.
18,19 In Singapore, these challenges are compounded by difficulties in communicating with healthcare providers because of language barriers, a fast-paced clinical environment, and experiences of receiving disrespectful remarks.
20,21 Navigating end-of-life issues is also a well-documented concern for patients,
22 and may be particularly difficult in the Singapore context, where cultural norms and taboos surrounding discussions of death present additional barriers.
23,24This study also highlights specific aspects of health coaching that patients found useful and suggests potential processes through which benefits are derived, namely, through the bolstering of the participants’ sense of control and security. While health coaching is often regarded as beneficial, little is known about why and how it works.
25 Our findings contribute to the literature by identifying potential mechanisms of action that represent promising directions for future research. These are consistent with previous research emphasising the centrality of control and security in the HF experience
26–28 and in other chronic diseases.
29–31The study also proposes several directions for strengthening future interventions. First, coaching content may be more personalised, with participants selecting topics aligned with their needs, readiness, and interests. Greater emphasis may be paid to practical, concrete, condition-specific guidance on integrating lifestyle adjustments. Second, coaching interventions may draw from salutogenic approaches like Local Area Coordination
32 to support patients with HF in envisioning and articulating what it means to lead a good and meaningful life, thereby addressing their needs for guidance on how they might forward in life following a health crisis. Third, given the existential tensions described, health coaches working with patients with HF should be trained not only in symptom management but also in recognising psychological distress and providing basic psychosocial support. This represents an area of need hitherto not adequately emphasised in existing health coaching competency frameworks.
33 Clear pathways for timely escalation to specialist psychosocial and palliative care services should also be established.
Limitations of the study include its single-centre design and its restriction to English- and Chinese-speaking participants, potentially excluding perspectives of patients from other linguistic and cultural backgrounds. In addition, despite efforts to recruit female patient participants for the interview, none agreed to participate. Consequently, all patient participants were male. While this reflects the predominantly male composition of the randomised controlled trial sample, the absence of female patient perspectives means that the findings should be interpreted with caution when considering applicability to female patients. As participation was voluntary, it is possible that those who agreed to be interviewed may have been more engaged or held more positive views of the programme than non-respondents. Finally, we were unable to recruit patient participants with NYHA class IV HF, as these patients tended to have a high symptom burden and were often too unwell to participate in research. As a result, the findings may not fully capture the experiences, needs, or priorities of patients with more advanced disease and their caregivers.
Despite these constraints, the findings have important implications for the design of health coaching programmes, underscoring the need to tailor content to patients’ informational, emotional, and existential needs and to equip coaches with the skills and training necessary to support this population effectively.