Introduction
Sexual harassment is a broad term that refers to unwelcomed verbal or physical sexual attention directed toward an individual.
1 It encompasses verbal and nonverbal gender-based behavior and is considered a global problem that threatens the basic human rights of both men and women.
2 Previous studies on sexual harassment in the medical community have highlighted the detrimental effects on the victims and bystanders.
3 Experiencing sexual harassment has been associated with poor mental and physical health, contributing to burnout, decreased psychological safety, and increased attrition in the physician workforce.
1,3 Moreover, failing to address unprofessional behavior in medical education risks passing these behaviors to the next generation of trainees, perpetuating a cycle of sexual harassment.
4,5A recent study of over 20,000 U.S. medical residents found that sexual harassment was frequently experienced by both female (24.8%) and male residents (3.2%), yet the majority chose not to report it despite being aware of reporting mechanisms.
6 Sexual harassment is recognized as a significant issue in the Japanese medical community, prompting hospitals and medical schools to establish institutions or committees for its prevention and management. A survey of Japanese medical residents revealed that 42.5% had experienced sexual harassment, with females disproportionately affected.
7 Beyond these high rates, a study that presented scenarios of sexual harassment to 1,000 primarily male Japanese staff physicians found that fewer than half knew how to appropriately respond.
8 The prevalence of sexual harassment among Japanese medical students during clinical clerkships remains unknown, and no studies have explored how students respond to such experiences.
To address this gap, we conducted a nationwide survey with first-year residents (recently graduated medical students) in Japan to examine the prevalence of sexual harassment and reporting patterns during ward training. Through this work we aim to elucidate the issue with the goal of creating supportive environments while establishing effective management systems for young doctors facing sexual harassment.
Results
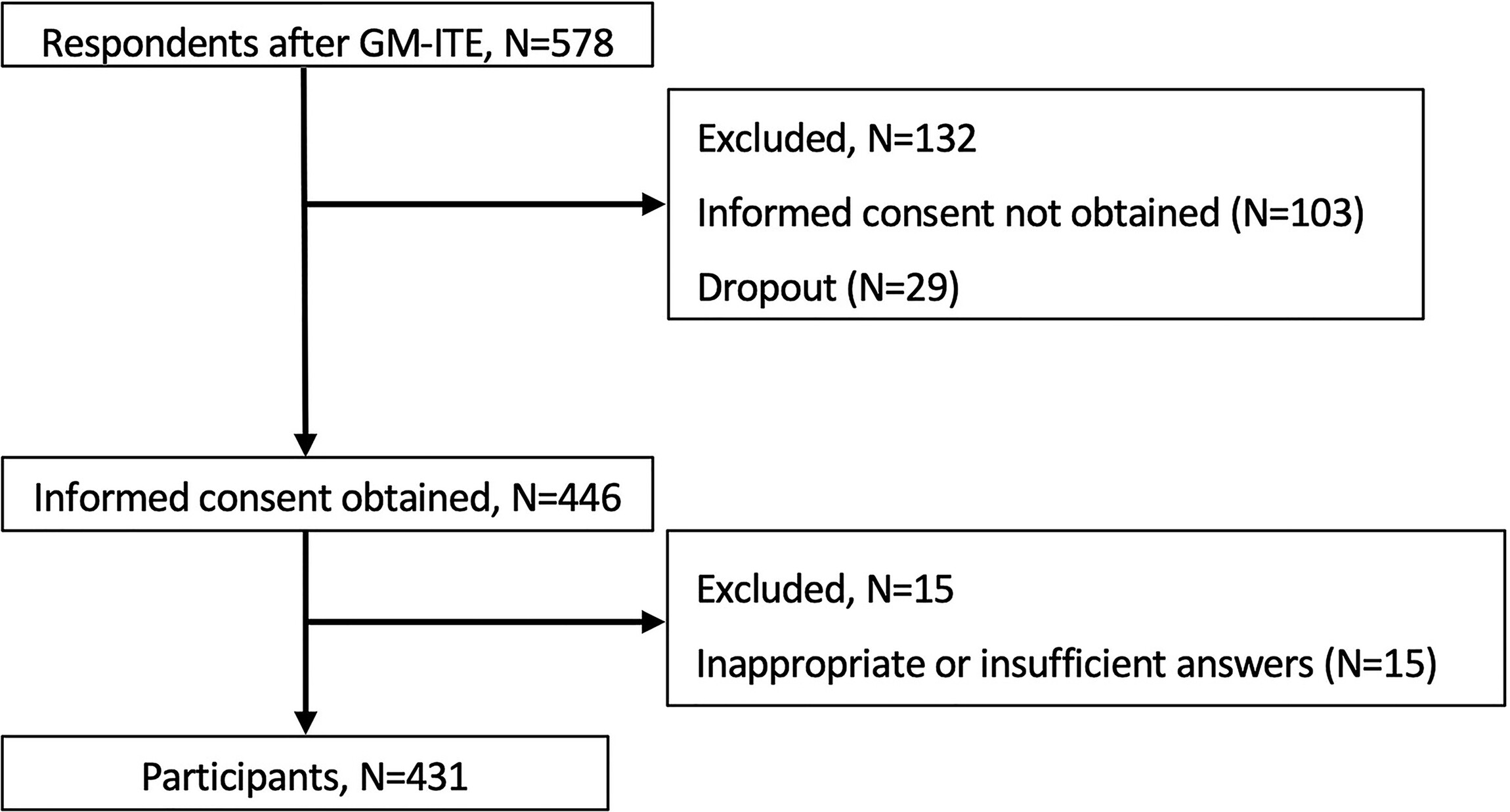
Of the 578 residents who participated in the GM-ITE, 431 assented and completed the study (response rate 74.5%) (
Fig. 1). Overall, the residents were men (71.2%,
N = 307) with an average age of 25.8 years (standard deviation 2.75 years).
Sexual harassment was experienced by 9.0% (
N = 39/431) of residents during their medical school clinical clerkships; 20.2% of women experienced sexual harassment (
N = 25/124), whereas 4.6% of men experienced it (
N = 14/307). Gender harassment was experienced by 7.4% (
N = 32/431) of residents during their medical school clinical clerkships, comprising 16.9% of the women (
N = 21/124) and 3.3% of the men (
N = 10/307). Sexual coercion was encountered by one male participant. Except for sexual coercion, the results were significantly higher for women (
p < 0.001) (
Table 1).
Among those who had experienced sexual harassment, 51.3% (
N = 20) of the residents reported having knowledge of formal reporting structures for sexual harassment. However, only two residents (5%) formally reported the sexual harassment incidents. Notably, 76.9% (
N = 30) of the residents stated they would not report sexual harassment (
Fig. 2).
Among those who experienced sexual harassment, nearly half (48.7%) disclosed the incident to others. The residents most commonly disclosed to friends (
N = 15, 78.9%) and teachers (
N = 5, 12.8%). The two respondents who did report sexual harassment to the designated departments consulted a friend and the perpetrator’s supervisor, respectively. Notably, none of the five residents who consulted their supervising teachers formally reported the incidents they had experienced. Of the 20 individuals who did not disclose to anyone, 19 participants stated that they would not have reported sexual harassment regardless of their knowledge about the reporting structures (
Table 2).
Discussion
To our knowledge, this was the first study to examine sexual harassment experiences of medical students in Japan during their clinical clerkships. Our results determined that nearly one in 10 (9%) medical students in Japan encountered sexual harassment during their clinical clerkships, and women experienced it significantly more often than men. Importantly, we found strikingly low rates of reporting, even among those who were aware of the reporting systems. In the absence of formal reporting, many students sought guidance, primarily from friends. However, even when teachers were consulted about sexual harassment, these interactions did not lead to formal self-reporting, underscoring the limited utilization of established reporting systems. These findings underscore critical gaps in the effectiveness and accessibility of current structures designed to address sexual harassment.
Interestingly, the rate of sexual harassment among medical students was relatively low compared to the previously reported rate of 42.5% among Japanese residents.
7 This discrepancy likely stems from Japan’s observation-based clinical training for medical students, which limits direct interactions with medical staff and patients compared to residency, reducing opportunities for sexual harassment.
10,11 However, as clinical training in Japan shifts toward more practical clerkships, understanding the risks of sexual harassment and barriers to reporting becomes increasingly important.
10A substantial proportion (76.9%) of those who reported experiencing sexual harassment stated they would not report it, regardless of their familiarity with the structures involved or the reporting methods. Although there were no gender differences in reporting behavior in this study, we consider it possible that the trend would change if the number of participants were increased. This finding underscores the persistent underreporting and social stigmatization of sexual harassment in Japan. The present study did not explicitly investigate the underlying reasons for non-reporting; however, several plausible explanations can be inferred. They include fears of differential treatment following disclosure, anxiety about disrupting interpersonal or professional dynamics within the workplace, and apprehension regarding potential retaliation, as has been reported in prior research.
12,13 Additionally, the reluctance to report may be reinforced by the just-world hypothesis—a cognitive bias wherein individuals, including the victims themselves, assume that outcomes are inherently deserved, thereby erroneously attribute blame to the victim rather than the perpetrator.
14 Such psychological and structural deterrents may contribute substantially to the silencing of victims and warrant targeted institutional interventions. Future studies should examine the reasons victims choose not to report sexual harassment to develop appropriately tailored approaches that strengthen reporting systems.
The majority of the students did not formally report their experience of sexual harassment but consulted others, especially friends and supervising teachers. Notably among those respondents who disclosed to their supervising teachers during clinical clerkships, none of the students subsequently formally reported the incident. This study did not assess the responses of supervising teachers consulted about sexual harassment, yet it does raise questions about the need for mandatory reporting and the need for preparing supervising teachers on how to better prepare and handle sexual harassment disclosures. Future work should also examine whether hospitals have established guidelines and protocols for addressing sexual harassment and assess the impact of these policies on harassment rates and reporting behaviors. Although this study was exploratory in nature, future research should employ multivariable models to identify key individual-level predictors (gender, age) of non-reporting and harassment experiences. Such analyses are critical to elucidate causal pathways and to inform effective, targeted interventions.
This study has several limitations. First, due to restrictions on the number of survey items, information regarding the perpetrators of sexual harassment was not collected. Previous studies have identified potential perpetrators as senior doctors, colleagues (including other medical students), patients, patients’ families, and allied medical staff.
7 Future research focusing on the characteristics of perpetrators may help develop strategies to protect medical students. Second, the number of respondents who encountered sexual harassment was small. Future studies should increase the overall sample size to confirm and refine our findings. Third, this study did not consider racial differences. More than 98% of medical students in Japan are Japanese because admissions, graduation, national examinations, and practical training are all conducted in Japanese. Therefore, from the perspective of diversity, we examined a population with a highly homogeneous social and cultural background. Finally, other issues to consider include recall bias (students reported experiences during medical school after graduation; memory may be imperfect), selection bias (only students who took the GM-ITE and agreed to participate were surveyed), and social desirability bias (even with anonymity, underreported harassment experiences is likely due to topic sensitivity).
Conclusions
Although 9.0% of first-year residents in Japan who responded to our questionnaire had encountered sexual harassment during their medical school clinical clerkships, only a small proportion (5.0%) chose to report it, whereas the majority (76.9%) indicated they would not report such incidents. Furthermore, approximately half of the residents who encountered sexual harassment engaged in consultative behavior with others (mainly friends and teachers); this did not lead all of them to report the incidents to formal departments. These results suggest potential high physical and psychological hurdles in reporting to a formal department, which were not clarified in this study. These findings reaffirm that reported sexual harassment cases represent only the tip of the iceberg. It is therefore crucial to investigate the reasons victims refrain from reporting and the obstacles they encounter when they do.
At present, there are no common rules against sexual harassment of medical students during clinical clerkships in Japan. This may be due to blurring of the boundaries for relationships and behavior, especially in highly specialized professions, with a background that makes it difficult for victims to understand the situation, as well as the taboo concerning talking about sexual harassment.
15 To prevent sexual harassment in the future, mandatory bystander training
16 and strengthening supervisor responsibility mechanisms
17 would be useful. Based on previous studies,
15–17 system improvement and implementation should be considered with regard to the cultural background of Japan. Addressing these issues is essential to fostering a safe and supportive environment where young doctors can develop both personally and professionally.
Authors’ Contributions
M.S. and T.W. conceptualized and designed the study, drafted the article, and provided administrative, technical, and material support. M.S. and T.W. secured study funding. V.S., E.M.V., Y.N., and Y.T. supervised the study. All authors were involved in data acquisition, analysis, and interpretation and had full access to all the data. All authors take responsibility for the integrity of the data and accuracy of the analyses. All authors critically revised the article for important intellectual content and read and approved the final article. All ideas presented in this study originated from the authors. Language editing was supported by ChatGPT to enhance clarity and readability, and all outputs were carefully reviewed and verified for accuracy by the authors.
Acknowledgments
A cohort of esteemed professionals substantially contributed to the success of the GM-ITE process. The authors extend their sincere gratitude to all members of the Examination Preparation Committee, their unyielding dedication and insightful contributions were instrumental to our analyses. In addition, the authors express their heartfelt appreciation to the exemplary individuals of the Examination Peer Review Committee, their meticulous oversight and constructive feedback strengthened the credibility and quality of the GM-ITE. The invaluable contributions of all the committee members were pivotal to this project’s success. The authors also extend their deepest gratitude to Juhei Matsumoto for his invaluable contribution to the management of the entire research process; his dedication and sincerity were instrumental in the success of this work. Finally, we acknowledge the invaluable guidance and support of Dr. Sanjay Saint, Dr. Nathan Houchens, and Ashwin Gupta from the University of Michigan Medical School, whose expertise and mentorship have significantly enriched the development and promotion of clinical research initiatives in Japan.