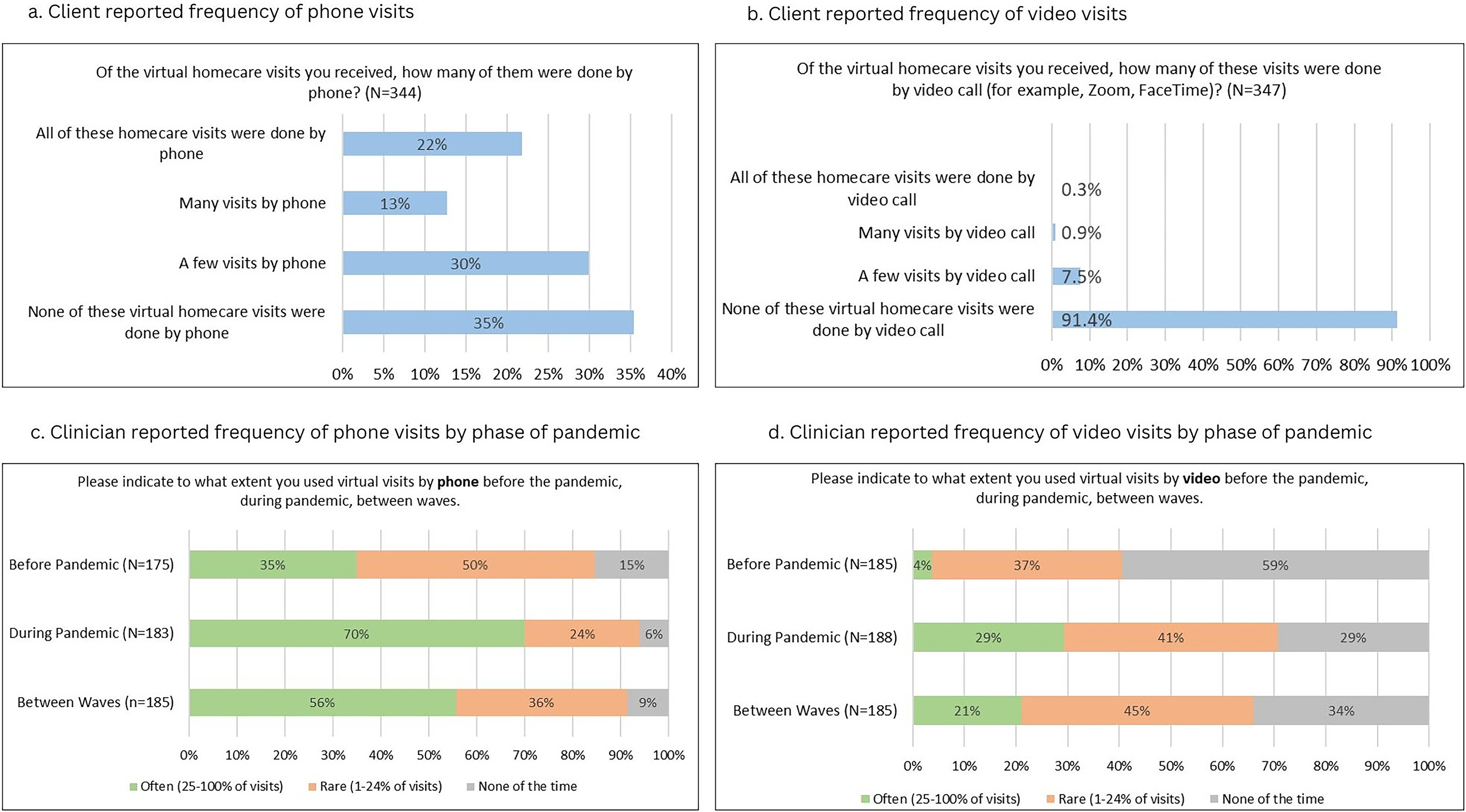
Frequency of virtual visits in palliative homecare
Half of the clients had experienced virtual visits (30% reported for a few of their visits, 20% for many of their visits), but, for the majority (65%), these virtual visits were by telephone. Only 8.7% reported any use of online video visits and, for 7.5%, this modality was only used for a few of their virtual visits (
Fig. 1a). Most clients (55%) reported that they were not often given the choice of having a virtual visit.
Clinicians reported a marked increase in the frequency of their use of virtual visits through pandemic peaks (
Fig. 1b), with a doubling in those using phones “often” and a seven-fold increase in using video visits “often.” However, even at pandemic peaks, 29% had never used video visits, 41% used these rarely and only 29% used video visits often, and this was not sustained beyond the peaks.
Multivariate regression analysis (
Supplementary Data S2) revealed significant differences in the frequency of phone visits across professions, during the peaks of the pandemic. Compared with physicians, nurse consultants, and nurse practitioners, health care aides were 60.3%
less likely to use phones often for virtual visits (
p < 0.001) and 20.8%
more likely to use phones rarely (
p = 0.041). Homecare nurses were 18.4%
less likely to use phones often (
p = 0.04), but 13.9%
more likely to use them rarely (
p = 0.032) compared with physicians.
Differences in video visits were observed across gender groups, urban–rural practice groups and provinces. Male clinicians were 16.4% less likely to have used video visits often compared with females (p = 0.013). Physicians serving urban areas were 16.7% more likely to use video visits often (p = 0.044), compared with clinicians in rural areas. Compared with clinicians from QC, those from AB, BC, and ON were 20.1%−22.4% more likely to have used phone visits often during the peak of the pandemic. BC clinicians were 17.1% less likely to have never used video visits.
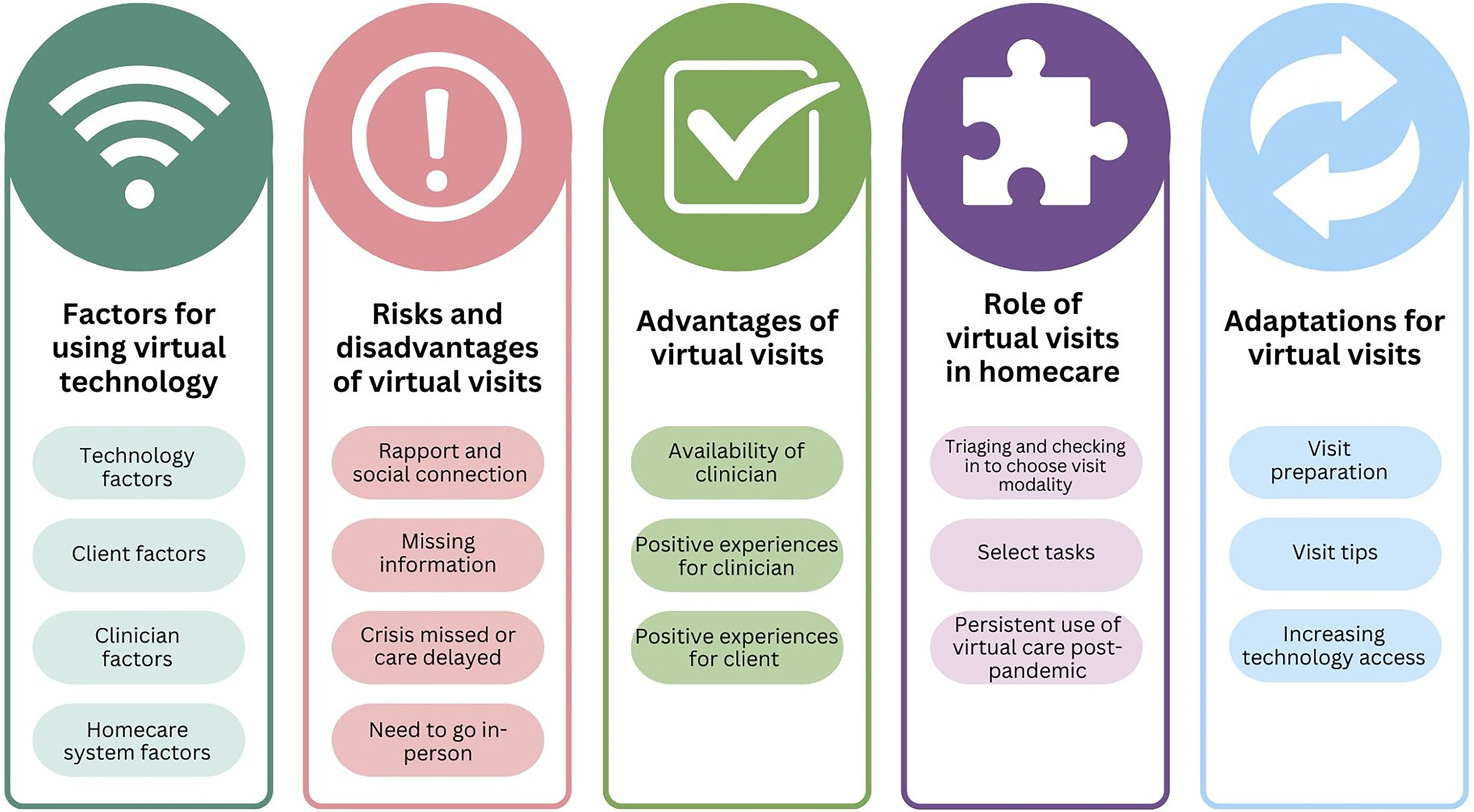
Factors for using virtual technology
Clinicians and clients identified certain prerequisites to be considered when deciding whether a virtual visit is appropriate. Subthemes include technology factors, client factors, clinician factors, and homecare system factors.
Technology factors
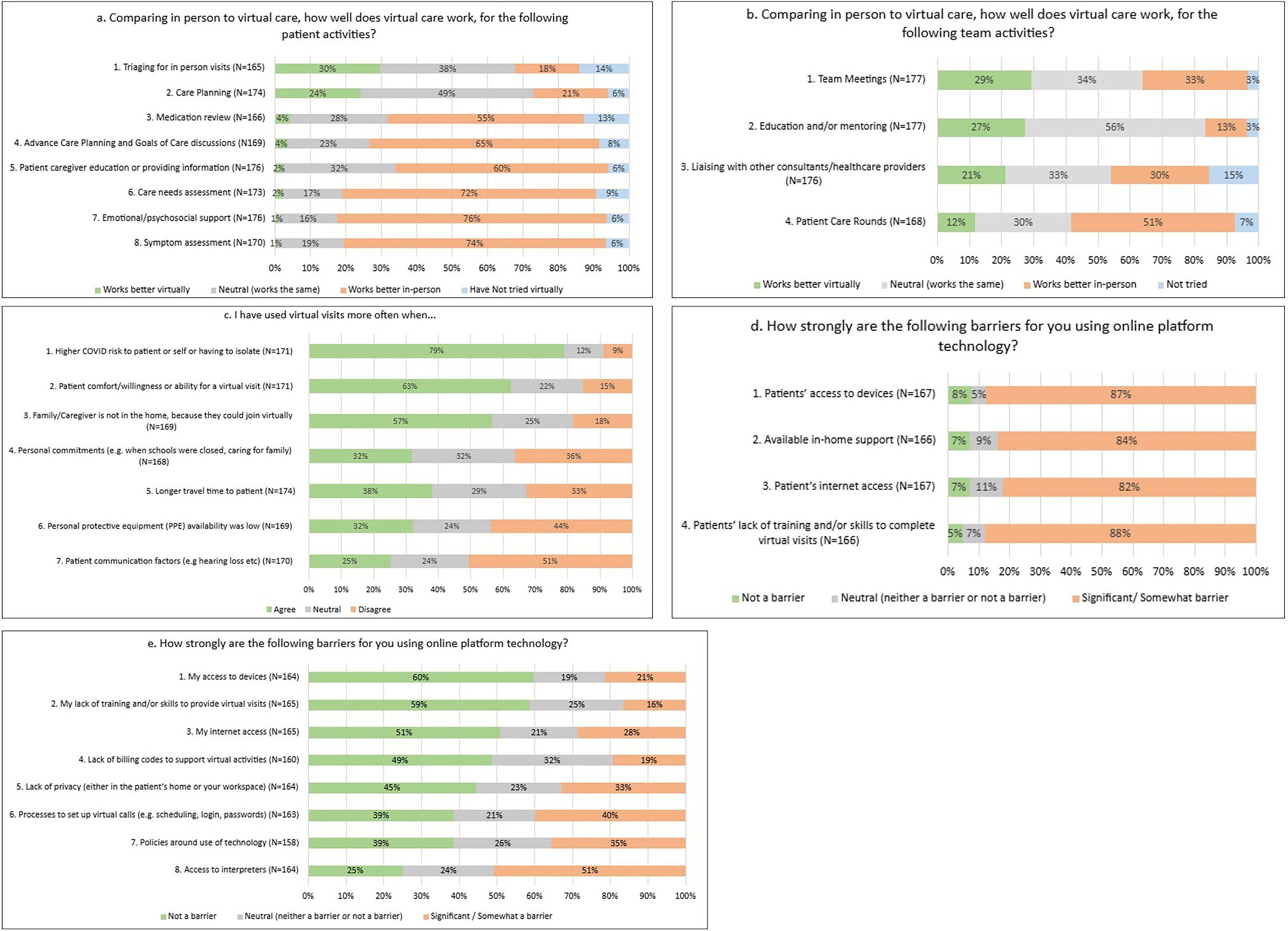
Challenges with using video visits for both clients and providers included Internet reliability, the need to recharge devices, and the availability of easy-to-use platforms. Internet reliability for clients was noted as a significant barrier (clients [39%] and clinicians [82%]). A clinician noted: “Inconsistent reliability of technology. So sometimes the Zoom feed, or the clients’ Internet would cut in and out or audio would lag. So that affects it too, the actual platform itself. Not always reliable” (Nurse5). Issues with technology such as battery life, security, Internet reliability, availability, and options for different tech platforms were reported: “And to just maintain the technology itself, right, booting and rebooting it, accessing things in multiple places that require extra passwords. Getting blocked out of the passwords, having to call IT and wait for that. That’s a start” (Nurse1).
In choosing when to use virtual technology, clinicians noted many challenges such as: “[There are] Expectations that technology works seamlessly in the community. It does not. significant time cost and is a barrier to communication. Clients dislike it. I am not saying do not use technology, I am saying use stuff that works and does not cost so much of our time. Also, there are no solutions to Dr. orders, other documents … . so paper charts still exist—very fragmented and confusing systems” (Open text—Clinician).
Client factors
Clients (44%) and clinicians (88%) found the limited ability of the client to use technology a significant disadvantage or barrier to virtual visits. From a patient’s perspective, “Again, it could have been sorted out if I could figure out how to maneuver a screen around so she could see, but I don’t know how to do that” (Patient1). Clinicians rated clients’ access to devices (87%) and Internet (82%) as significant barriers, but their own Internet access and device access were not often a barrier to using virtual visits (<29%). “I work in an indigenous community. Internet & phone services are challenging. The signals can be poor. The people often are unable to afford Internet services & may use pay-as-you-go cell phones” (Open text—Clinician). In an interview, a social worker noted socioeconomic inequities, “And the only ones you’re having the video calls with are the higher functioning with the money to have—so, the ones who have less money or less technology and less cognitive ability aren’t actually online.” Clients (47%) and clinicians (84%) reported requiring extra assistance from family caregivers to make virtual visits possible a significant barrier. Regression analysis indicated that clients aged ≥65 years were 19.9% more likely to report that they can only participate in virtual visits if someone is at home to help them (p < 0.001), compared with clients <65 years.
“The biggest factors are do they have a family or support system who can operate or use the technology for them? I think that’s the biggest one. We’ve definitely had situations where you have, say, an elderly, isolated client who is not even particularly comfortable on the phone and they can’t set up the Zoom, they don’t know how to do that. I think we have to be aware of that […] And, again, I don’t know that that was always a positive, sometimes it may have put them in a position where they perhaps wanted more privacy but needed the help with the technology.” (Specialist palliative nurse2).
Clinicians and clients expanded on client cognition, disabilities, education, and equity issues factoring into whether video visits could be used. For example, a clinician expressed that virtual visits can be an added source of pressure for people who are heard of hearing: “And then, of course, we have patients who are hard of hearing or aren’t comfortable with technology who found, and definitely expressed that being asked to use Zoom was a massive added pressure or thing that caused them to worry or get upset, because they really didn’t know” (Specialist palliative nurse2) and from a client (open-text), “I am not comfortable with technology, and I am not necessarily eager to learn at 75 years old.”
Clinician factors
In contrast to their assessment of clients’ technology skills, only 16% of clinicians rated their own training and skills for using online platform technology as a barrier. Clinicians were split on rating the ease of processes to set up virtual calls (e.g., scheduling, login, passwords), as 39% reported it as not being a barrier, 21% were neutral and 40% said it was a significant/somewhat of a barrier. Qualitative results were concordant with the quantitative split, a social worker noted, “I don’t think anybody on our team is bothering with Zoom calls to clients. It takes too much effort and bother”, while others were comfortable using virtual visits, “I don’t know, I like using more and more tools because it can supplement our knowledge. And I don’t know, I think it makes things a little bit easier. Sometimes, not always, but sometimes” (Nurse3). Clinicians were also split on whether they used virtual visits more often when they had personal commitments (e.g., when schools were closed or caring for their own family) as 32% said they agreed, 32% were neutral, and 36% disagreed.
Homecare system factors
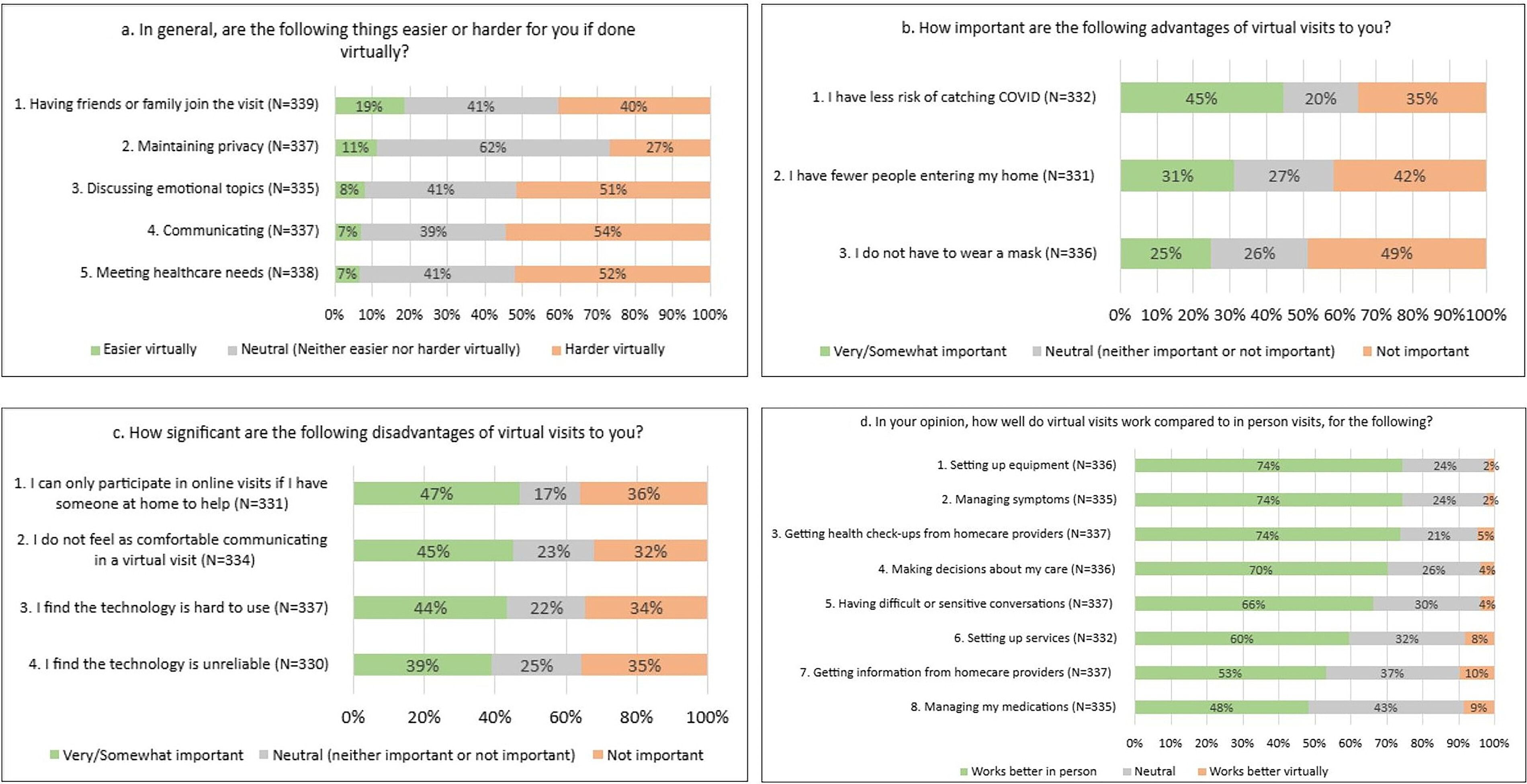
COVID-19 was a major contextual factor in determining the use of virtual visits. Considering COVID, 45% of clients and 79% of clinicians reported that the decreased risk of transmission was a very/somewhat important advantage of virtual visits. However, only 31% of clients reported that having fewer people entering their home is an important advantage of virtual visits and not having to wear a mask was not an important advantage of virtual visits for 49% of clients. The availability of PPE was not a barrier for 44% of clinicians. COVID drove some clinician decisions to use virtual visits: “And we use that a lot more, especially now, well, since COVID started because, obviously, we’re trying to reduce our footprint in our clients’ homes, because they are definitely part of the immunocompromised population” (Nurse3). However, clinicians noted difficulty in transitioning from paper to electronic documentation. Clients recognized how virtual visits were necessary to fill gaps during the pandemic: “The COVID pandemic and health care worker shortage changed the way health care and palliative services are delivered to patients. Is it ideal? Maybe not. But it’s the best the system can provide until alternative care is created” (Open text—Client). Another system factor was the dispersed nature of homecare work, with staff needing to work in a central office and a spread of client homes. One nurse noted, “If it’s something that’s urgent I usually will help someone over the phone and then try to see them within that day. But sometimes if they’re an hour one way from the office it may not be possible that day” (Nurse4). Participants also reported general staffing shortages as a barrier to virtual visits, “I think the barrier is just the busyness of the RNs and lack of staffing” (Nurse4).
Risks and disadvantages of virtual visits
Overall, most palliative homecare activities were rated as harder to do virtually by both clients and clinicians (
Figs. 3 and
4). Both clients and clinicians acknowledged that the information obtained from a virtual visit was not sufficient for safe, high-quality care. The subthemes were
Rapport and social connection,
Missing information,
Crisis missed or care delayed, and the
Need to go in-person.
Rapport and social connection
Key disadvantages of virtual visits, whether by phone or video, were in building rapport and sustaining social connections. Both clients and clinicians valued being physically present for relationship building. Clients (54%) felt it was generally more difficult to communicate virtually and having difficult or sensitive conversations was easier in person (66%). A client responded: “Feels less personable. Very impersonal. No human contact makes you feel like it is more of a question-and-answer session. Lack of human compassion” (Open text-Client). Clinicians (76%) also felt that emotional and psychosocial support worked better in person as a social worker said: “the difference in rapport, in connection, in feeling heard and seen is—you can’t even quantify the difference when you’re there and somebody gets to know you and see you and feel like they had somebody on their couch with them.”
Some clients (45%) did not feel as comfortable communicating in a virtual visit and clinicians appeared to recognize this, as 63% clinicians reported using virtual visits more frequently if the patient was comfortable/willing to have a virtual visit. Regression analysis revealed that clients aged ≥ 65 years are 4.9% less likely to report that communication is easier during virtual visits (p = 0.033), 9.3% less likely to be neutral (p = 0.012), and 14.2% more likely to report that communicating is harder during virtual visits (p = 0.014) compared with clients aged <65 years.
Missing information
Qualitatively, clinicians were quite concerned about missing information when not in the client’s home. Clinicians reported missing some critical sensory information such as client’s nonverbal cues, smells, and details of the home environment as a major disadvantage of virtual visits, “Much is missing virtually; palliative care of clients requires all of our senses—from the moment we walk into the home to where we see the client. Seeing the home, seeing the support people, the client from head to toe, the surroundings, the smells, noises and other—is important in overall care of the palliative client at home” (Open text—Clinician). Additionally, clients were noted by clinicians to sometimes minimize symptoms virtually. A social worker reported that she witnessed a client minimizing their issues to the physician: “The doctor would have set up a phone appointment, and sometimes I’ m there for them. And you’re like, “Holy cow. You have no idea.” If I wasn’t here to give the other side of that, you’d believe her. And no, this is why we’re ending up with so many scenarios where we’re having way more crises than we should have because it’s missed. They just had no idea that things had slid or were that much different because people will do the, “Oh, yes, I’ m good,” so frequently.” Clients noted the dangers also, “When you are hearing impaired or vocally impaired …can get confusing or may hear or interpret the information given improperly. Room for inaccuracy. This can lead to false diagnosis over the phone or misinterpretation of my symptoms” (Open text—Client).
Crisis missed or care delayed
As a consequence of missing information when virtual visits were used instead of in-person care, participants shared stories of critical changes in client’s health being missed or care being delayed. “What ends up happening is when a client’s health is failing, we only tend to notice or hear about it when it has reached a crisis” (Open text—Clinician). Patient safety assessments were also harder virtually, as this nurse manager related intimate partner abuse, “Not much on paper…But he later beat the crap out of her. She was hospitalized. She had to flee. She ended up leaving that city. So that’s not going to be captured over the phone doing question A to B to Z. And there’s so many things, right? I’ m responsible for my safety, her safety and the staff I authorized to go in there. That’s not captured over the phone. There’s no way I believe that would be captured. So, a huge disservice to everybody” (Nurse5).
Need to go in person
From these risks and disadvantages, the need to go in-person emerged as central to certain types of palliative homecare tasks. For example, physical examination and hands-on-nursing-care, the initial homecare visit, interpretation and signing of documents were all tasks clinicians struggled to achieve with virtual visits. “So in person, we have lots of skills that we have to do with our clients. Things like, I don’t know, maybe enema administration, wound care, subcutaneous site changes, like physical skills, so you have to go and do those visits.” (Nurse3). Physiotherapy or occupational therapy were also required in-person, “If it’s something actually hands-on. If I’ m going or if someone’s coming to me, it’s usually like a physiotherapist, and she’s helping me with different exercises or manipulating parts of my body that I can’t anymore.” (Patient1).
Participants emphasized that it is essential for the first palliative homecare visit to be done in-person as it builds rapport, and clinicians can get a full assessment of the patient and their environment: “Only doing virtual visits as a follow up to an in-person visit. New consults are too challenging as you need to get into the home to get a sense of the real situation” (Open text—Clinician).
Clinicians reported (51%) that access to interpreters was an additional significant barrier when using virtual visits. A qualitative response explained: “…in an in-person visit, if I have someone that English isn’t their first language and they want to use a translator, I can phone the language line and I as usual, put them on speaker phone in the visit. Which isn’t as good as an in-person translator, but it’s what we have. But if I’ m doing it by Zoom, we don’t have an option, it’s way more complicated to call in an interpreter.” (Specialist palliative nurse2).
Advantages of virtual visits
Overall, clients and clinicians rated a few aspects of virtual care positively (
Figs. 3 and
4). One advantage noted was the increased
availability of clinicians enabled by virtual technology (e.g., clients being able to text case managers or phone to ask questions quickly). Beyond the lower infection risk for both clients and clinicians during virtual visits, other advantages reported within the subthemes were
positive experiences for clinicians and
positive experiences for patients.
Availability of clinicians
Clients mentioned they could connect with their health care providers faster and after hours: “Sometimes we need advice from the nurse, and it was more efficient to do so by phone call. My mom’s health declined quickly, and we needed nurses to care for my mom without much notice” (Open text—Client). The efficiency benefits of virtual care were recognized by clients, “So it was a perfect example of virtual that didn’t take as much time as her having to make a house call, and it was just as satisfying for both of us, and we put in place the things that we needed without any hesitation.” (Caregiver3). Of note, only one-third of clinicians reported an increase in their use of e-mails (29%) and text messages (31%) with clients once the pandemic started.
Positive experiences for clinicians
Reducing travel time to see patients was a benefit for some clinicians (38%). Other positive virtual experiences for clinicians included easier/faster communication between colleagues (e.g., transfer of care between clinicians, nurse to physician texting, clinician peer support and mentorship). With the pandemic, clinicians (53%) increased their use of e-mails and text messages (54%) between providers.
Efficiency of clinician education and virtual team meetings were also described as benefits of virtual modalities, for example, “So I’ m not asking them to give up 30 minutes on either side to come somewhere, you just show up at the time of the visit, we can have you contribute your piece and then off you go. So, I think it is definitely timesaving as well, so it gives an opportunity to, I think, include more people and collaborate differently” (Specialist palliative nurse2). Quantitatively, however, clinicians were split on whether team meetings were better in-person (33%) or virtually (29%) with 34% neutral, and 3% who had not tried virtual team meetings. Health care aides were 28% less likely to report that team activities worked better virtually compared with other professionals (p < 0.001). There were some provincial differences, compared with QC clinicians from ON reported that they were 18.9% more likely to report that team meetings work better virtually, 15.7% less likely to report that team meetings work better in-person and 3.3% less likely not to have tried a virtual team meeting. AB and BC were no different to QC.
Positive experiences for clients
One advantage noted qualitatively was that it was easier for family and friends to join the visit virtually: “The family conference. The getting everybody on the same page, hearing the same information, that was really useful, especially for the out-of-town family members and stuff. There are some really good uses of it” (Social worker1). Clinicians (57%) used virtual technology more when the caregiver or family member was not in the home so that they could include them in the visit. However, 40% of clients reported it was harder virtually to have friends and family join the visit than to have them in-person in the home. Other positive aspects of virtual visits for clients included convenience, saving their time and energy, not taking up space in the home, and being able to record the conversation. A virtual visit was “Easier to fit into the day, allowed my mom to sleep in because less prep time, didn’t have to ramp up to having company preparations, less stressful for mom having a day off instead of an appointment” (Open text-Client).
The role of virtual visits in homecare
Despite the described risks and disadvantages of virtual visits, checking in to choose the visit modality and select tasks emerged as aspects that could be done well virtually. We also heard about potential roles in the persistent use of virtual technology beyond the pandemic.
Checking in to choose the visit modality
Of all surveyed activities, clinicians noted that virtual visits worked better than in-person for triaging (30%) and for care planning (24%). Qualitatively, both clients and clinicians explained that a phone call was sufficient when the client was stable, with the caveat that the provider could switch from a phone visit to an in-person visit if the patient was not doing well. For example, when triaging visits, “If I phoned them in the morning, and they say, “You know what, everything’s fine. We don’t have any concerns, there’s no symptomatic issues,” then we might just leave it for another time” (Nurse3).
Clients noted it was helpful to have someone check in when things were not urgent: “Like, if I have a symptom and it’s not urgent, I don’t need someone to check on me, but I need someone I need to talk to a nurse to be, like, do I have to go to the hospital or should I—when do I go to the hospital? So, in that case, the virtual” (Patient2).
Professional roles factored into whether virtual care was perceived to have a role in triaging. Health care aides work is almost all “hands on” and regression analysis revealed health care aides were 29.1% less likely to report that triaging works better virtually (p < 0.001), 40.4% less likely to stay neutral on whether triaging works better virtually or in person (p < 0.001), and 88% more likely not to have tried virtual visits for triaging (p < 0.001), compared to physicians and palliative care nurse consultants. Provincial differences were also found on regression analysis with clinicians in AB and ON about 23% more likely to report that triaging works better virtually than in-person, while clinicians in all other Canadian provinces were 10.2%−11.6% less likely to report that triaging visits work better in-person.
Select tasks
Certain tasks were identified as well-suited to virtual visits, such as client education, communication about available supports and resources, and enabling external clinicians, such as the client’s oncologist or family physician, to join in the home visit. Overall, clients and clinicians favored in-person homecare and thought virtual modalities should be used only as a supplement to in-person visits.
“From my point of view as a caregiver, it is essential that certain visits are made in person for a better overall assessment of the situation and the risk assessment” (Open textClient).
“Other than phone calls to stable clients, palliative care needs to have visits in the home to establish relationships and provide well rounded care to the client; as mentioned, all of our senses are involved in palliative care. We are not going in to do one specific task; it is multitude of care in palliative care. I have been doing this work for more than 20 years” (Open text -Clinician).
Persistent use of virtual technology beyond the pandemic
A few clinicians felt that having the option of virtual care was important moving forward post-pandemic: “I had hoped we would continue virtual visits and move forward versus backwards to the old way of doing things… tradition and authority without much thought put into how things can work better, more efficient, more effective without compromising patient care, better work life balance, etc.” (Open text — Clinician).
Beyond the pandemic, 36% of clients wanted some/most of their visits to be virtual, 16% had no preference, but 48% wanted none of their visits to be virtual. Regression analysis revealed that both levels of education and age are associated with these preferences. Older adults aged ≥65 years were 21.5% less likely to prefer some or most visits to be virtual (p < 0.001) and 22.3% more likely to want none of their visits to be virtual compared with clients <65 years (p < 0.001). Clients with <grade 12 (high school) education were 16.4% less likely to prefer some or most virtual visits (p = 0.004), and 19.4% more likely to want none of their visits to be virtual beyond the pandemic, compared to those with post-secondary education (p = 0.008).
Adaptations for virtual visits
Clients and clinicians provided suggestions on how virtual visits could work more seamlessly. These included: visit preparation, increasing technology access, and visit tips.
Visit preparation
Clients noted the importance of planning ahead for a virtual visit by creating a list of questions for the clinicians: “I have my list of medications ready. I have a list of pertinent symptoms ready. I like to keep a list of questions on hand too” (Open text—Client). Older clients noted the need to have a caregiver in-person to help with set up of the virtual visit and for general technology support around the appointment.
Clinicians also noted the importance of preparing ahead.
“So I would try and consider that beforehand and say OK, let’s look at the capacity of doing virtual, how can we make this the best experience possible. Testing the sound system and testing whatever sound system you’re using and whatever. Like if it’s the phone, do they need to have an interpreter to speak to that individual. They’d probably be best served by having someone who can interpret for them, like even the language. […….] The patient’s or client’s comfort level with technology, that’s the first thing you need to know” (Nurse2).
Increasing technology access
Clients and clinicians both suggested that increased flexibility for using e-mail and text communication, or other types of technology that clients use regularly and are already familiar with, would improve virtual visits. “At this time, we are not to communicate via e-mail with non-[Organization] providers or even client’s and family members. This is not sustainable. Email/text communication is especially useful when we’re dealing with a language barrier” (Open text — Clinician).
Visit tips
Privacy of virtual visits was not a concern for the majority of clients (62% were neutral on whether virtual visits made it harder to maintain privacy, 27% rated it harder and only 11% rated it easier) and 45% of clinicians felt privacy in the client’s home was not a barrier for using online platforms. They did note some adaptations to maintain privacy “[…] it’s important to ask who is in the room as there might be family members you cannot see on camera” (Open text—Clinician).
Participants also suggested recording the virtual visit to ensure clients can go back and listen if needed and share the recording with family members and other people who were not able to make it to the appointment: “I like the recorded [conversations]. That’s a nice thing to be able to have the family member record that so somebody else can hear what was said, so we’re all on the same page. Those things are really good add-ons in the recent years” (Social worker1).
Other tips resonating with the themes already described included making sure the client has a caregiver present in-person during virtual visits, and having the first client–clinician visit in-person before beginning virtual visits. Synthesizing the themes, we created clinician and client tip sheets (
Fig. 5).