

Impact of Early Life Stress on Neurobiological Vulnerability to Obsessive-Compulsive Disorder: Early Life Stress & Neurobiological OCD Risk
Abstract
The impact of early life stress on neurobiological vulnerability to obsessive-compulsive disorder (OCD) is a major focus of psychiatric research. Individuals with OCD frequently report that psychosocial stress exacerbates their symptoms, with many attributing the onset of symptoms to stressful life events. However, the exact pathophysiological relationship between stress and OCD is not well understood. Stress has been shown in preclinical studies to have significant effects on cortico-striatal and limbic circuitry, including neuronal atrophy in the frontal cortices, dorsomedial striatum, and hippocampus, as well as neuronal hypertrophy in the dorsolateral striatum and amygdala. These neurobiological effects may contribute to an imbalance between goal-directed and habitual behaviour, which is associated with OCD symptoms. Furthermore, genetic and environmental factors, including early life stress, play an essential role in the advancement of OCD. Understanding gene-environment interactions and pathogenic mechanisms is critical to advancing precision medicine and improving treatment outcomes for OCD and related disorders. This review emphasises the need for additional research into how early life stress interacts with genetic factors to cause the behavioural, cellular, and molecular changes seen in OCD. Integrating global mental health and translational neuroscience approaches shows potential for enhancing our understanding and treatment of OCD and related disorders.
1 Introduction
Obsessive-Compulsive Disorder (OCD) is a significant mental health concern because of its prevalence and the considerable impairment it can impose on individuals [1]. It is a cornerstone in the spectrum of obsessive-compulsive and related disorders (OCRDs), shedding light on a broader group of conditions marked by intrusive thoughts and repetitive behaviours. OCD is defined by the presence of obsessions and/or compulsions, which manifest as repetitive,
| ACC | Anterior Cingulate Cortex | mPFC | Medial Prefrontal Cortex |
| ACT | Acceptance and Commitment Therapy | NMDA | N-methyl-D-aspartate |
| ALIC | Anterior Limb of the Internal Capsule | OCD | Obsessive-Compulsive Disorder |
| CBT | Cognitive Behavioral Therapy | OCRD | Obsessive-Compulsive and Related Disorder |
| CSTC | Cortico-Striatal-Thalamo-Cortical | OFC | Orbitofrontal Cortex |
| CT | Cognitive Therapy | PET | Positron Emission Tomography |
| DBS | Deep Brain Stimulation | PFC | Prefrontal Cortex |
| DSM | Diagnostic and Statistical Manual of Mental Disorders | PTSD | Post-Traumatic Stress Disorder |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, | SSRI | Selective Serotonin Reuptake Inhibitor |
| 5th Edition | SNP | Single Nucleotide Polymorphism | |
| DTI | Diffusion Tensor Imaging | tDCS | Transcranial Direct Current Stimulation |
| EX/RP | Exposure and Ritual Prevention | TMS | Transcranial Magnetic Stimulation |
| fMRI | Functional Magnetic Resonance Imaging | TS | Tourette's Syndrome |
| GWAS | Genome-Wide Association Study | VC/VS | Ventral Capsule/Ventral Striatum |
| mFC | Medial Frontal Cortex | VRET | Virtual Reality Exposure Therapy |
intrusive, and undesirable thoughts, pictures, impulses, or urges accompanied by anxiety. Compulsions, on the other hand, manifest as recurrent behaviours or mental acts prompted by an individual's attempt to alleviate the distresscaused by obsessions or to achieve a sense of completion [1,2] such as washing, checking, counting, and repeating specific procedures.
Cognitive-behavioral theories are essential to the understanding of OCD, emphasising the relationship between obsessions and compulsions [2]. Traditionally, obsessions have been thought to play a fundamental role for increased stress or discomfort, resulting in compulsive behaviours in an attempt to alleviate misery. However, new evidence challenges this approach, indicating that compulsions may precede obsessions, with obsessions evolving as post-hoc justifications for these actions. This alternative viewpoint calls for further research to understand the nuanced dynamics of obsessions and compulsions within the OCD spectrum. Furthermore, OCD frequently overlaps with concomitant illnesses, confounding the clinical presentation and therapeutic trajectory [3]. Anxiety disorders, depression, and other OCRDs are common comorbidities, adding to the burden of the disease and emphasising the importance of holistic and integrated care. Furthermore, OCD can have a significant impact on several domains of functioning, including the social, occupational, and relationship realms [4]. The prevalence of OCD highlights the need for personalized therapies that address the many levels of impairment reported by affected individuals.
Given the complexities of OCD, it is critical to appreciate the individual experience of those suffering from the illness. Many people with OCD are acutely aware of the severity of their obsessive symptoms and have a strong desire for further control over their actions. This insight emphasises the distress and impairment caused by OCD, beyond mere symptomatology to reflect the significant psychological and emotional toll exacted by this disorder [5]. The contextualization of OCD goes beyond its individual manifestations to include broader societal and cultural aspects. Misconceptions and stigma surrounding OCD can compound the difficulties that people have when seeking understanding and support. Furthermore, cultural influences on the presentation and perception of OCD symptoms might influence aid behaviours and treatment preferences. Thus, a thorough understanding of OCD demands a diverse lens that considers not just its clinical manifestations but also its societal implications.
Furthermore, OCD is usually associated with comorbid disorders, complicating both clinical presentation and therapeutic trajectory. Anxiety disorders, depression, and other OCRDs are prevalent comorbidities that contribute to morbidity and death, emphasising the significance of comprehensive and integrated management. Furthermore, OCD can have a significant influence on multiple domains of functioning, including the social, occupational, and relationship realms. The prevalence of OCD highlights the need for personalized therapies that address the multifaceted dimensions of impairment reported by affected individuals.
Current studies seem to be critical in expanding our understanding of the intricacies of OCD, including etiological variables, treatment approaches, and prognostic markers. Researchers attempt to uncover the intricate mechanisms behind OCD pathology by employing a variety of approaches encompassing the neurobiological, genetic, and psychosocial realms. Furthermore, OCD is usually associated with comorbid disorders, complicating both clinical presentation and therapeutic trajectory. Anxiety disorders, depression, and other OCRDs are prevalent comorbidities that contribute to morbidity and death, emphasising the significance of comprehensive and integrated management. Furthermore, OCD can have a significant influence on multiple domains of functioning, including the social, occupational, and relationship realms. The prevalence of OCD highlights the need for personalized therapies that address the multifaceted dimensions of impairment reported
by affected individuals. Current studies seem to be critical in expanding our understanding of the intricacies of OCD, including etiological variables, treatment approaches, and prognostic markers. Researchers attempt to uncover the intricate mechanisms behind OCD pathology by employing a variety of approaches encompassing the neurobiological, genetic, and psychosocial realms. Furthermore, clinical trials assessing the efficacy of pharmacological and psychotherapy therapies attempt to improve treatment outcomes and quality of life for those suffering from OCD.
2 Understanding Stress, Trauma & OCD
Several environmental events, such as perinatal and childbirth complications, age-related changes in reproductive systems, parental trying to raise styles, socioeconomic problems, and physiologic insults or injuries, have been identified as potential contributors to OCD, many of which can be considered stressful in a broad sense [6]. These stresses combine with underlying vulnerability characteristics, contributing to the complicated aetiology of OCD and other neuropsychiatry disorders [7]. The term "stress-diathesis" interaction emphasises the dynamic interplay between stressors and inherent vulnerabilities in the development of psychopathology [8]. In some instances, stress may directly precipitate the development of OCD symptoms, while in others, it may serve to activate latent vulnerabilities, or exacerbate existing symptomatology. Importantly, the type and severity of stressors may influence the manifestation of OCD symptoms, highlighting the heterogeneous nature of the disorder.
Stress, particularly psychosocial stress and exposure to traumatic events, has been implicated in the onset and exacerbation of OCD symptoms [2, 6]. Acute stressors have been shown to induce obsessionally in both healthy and psychiatric populations, with a significant proportion of OCD patients reporting stressful life events preceding the onset of their symptoms. Longitudinal studies further support a causal association between stressful life events and the development of OCD symptoms, although the possibility of recall bias underscores the need for cautious interpretation [9]. Trauma, as an extreme form of psychosocial stress, has also been linked to increased OCD symptom severity and elevated risk for the development of OCD. Childhood traumatic events have been associated with heightened OCD risk in adulthood, underscoring the enduring impact of early-life stressors on psychopathology.
Furthermore, trauma survivors may experience overlapping symptoms of OCD and posttraumatic stress disorder (PTSD), implying that the two disorders share underlying mechanisms. However, the specificity of stressors in contributing to OCD symptoms is still being debated. While some studies suggest a disease-specific contribution of stress to OCD symptoms, others propose a more non-specific vulnerability factor, such as neuroticism, that may underlie stress reactivity across various mood and anxiety-related disorders [1, 8]. More research comparing the effects of stress across different clinical conditions is needed to understand the unique contribution of stress to OCD pathogenesis. Operationalizing trauma presents a challenge because not all potentially traumatic events are subjectively perceived as traumatic by individuals, and subjective trauma experiences may differ from DSM-5 criteria. Nonetheless, stressful life events thought to have precipitated the onset of OCD may be subjectively perceived as traumatic, influencing symptom presentation and course. The subjective experience of trauma, rather than its diagnostic accuracy, appears to be a key determinant of its impact on psychopathology, emphasising the complexity of stress-stimulated symptomatology [6].
Understanding the subtle relationship between stress and OCD symptomatology has the potential to inform personalised interventions and improve treatment outcomes for affected people. Aside from stress-induced symptomatology, recent research has looked into the potential mechanisms underlying the impact of stress on OCD pathogenesis. Neurobiological studies have revealed changes in stress-responsive neural circuits such as the amygdala, prefrontal cortex, and hippocampus, which may contribute to the development and maintenance of OCD symptoms in the presence of stress. Furthermore, molecular studies have identified dysregulation of stress-related neurotransmitter systems, such as serotonin and dopamine, implying neurochemical imbalances at the stress-OCD interface [10]
Furthermore, psychosocial factors such as maladaptive coping strategies and interpersonal stressors can amplify the impact of stress on OCD symptoms. Individuals with OCD may experience heightened interpersonal sensitivity and maladaptive perfectionism, which can amplify the distress associated with stressors and maintain symptom severity [11]. Furthermore, the presence of comorbid conditions, such as depression and anxiety disorders, may compound the effects of stress on OCD, emphasising the importance of comprehensive assessment and integrated treatment approaches.
Emerging evidence suggests that early intervention strategies targeting stress management and resilience-building may confer protective effects on the development or exacerbation of OCD symptoms [1,10]. Psychotherapeutic modalities, such as cognitive-behavioral therapy (CBT) and mindfulness-based interventions, have shown promise in providing individuals with coping mechanisms to better navigate stressors and reduce the impact on OCD symptoms. Furthermore, pharmacological interventions targeting stress-related neurobiological pathways, such as selective serotonin reuptake inhibitors (SSRIs) and glutamatergic modulators, may offer adjunctive benefits in reducing OCD symptoms in the context of stress.
3 Potential Mechanism for Stress Effects on OCD Symptoms
Understanding how stress affects the manifestation of obsessive-compulsive disorder (OCD) necessitates delving into the complex interaction of stress, brain structure, and behaviour. Both acute and chronic stress can profoundly impact an individual's cognitive and behavioural processes, frequently tilting the balance towards rigid, habit-like patterns of behaviour while impairing flexible, goal-directed learning and control [12,13, 14]. This observation is particularly relevant in the context of OCD, as an overdependence on habit may contribute to the
development and maintenance of symptoms [15]. Preclinical research has provided valuable insights into the neurobiological basis of stress-induced behavioural changes. Studies suggest that stress can induce structural and functional changes in cortico-striatal and limbic circuits, which are critical for regulating habitual and goal-directed behaviours. Excessive stress has been linked to neuronal atrophy and synaptic loss in key brain regions such as the prefrontal cortex (PFC), hippocampus, and striatum, as well as impaired neurogenesis in the hippocampus (Figure 1). In contrast, stress can lead to neuronal hypertrophy and synaptic potentiation in regions such as the amygdala and dorsolateral striatum.
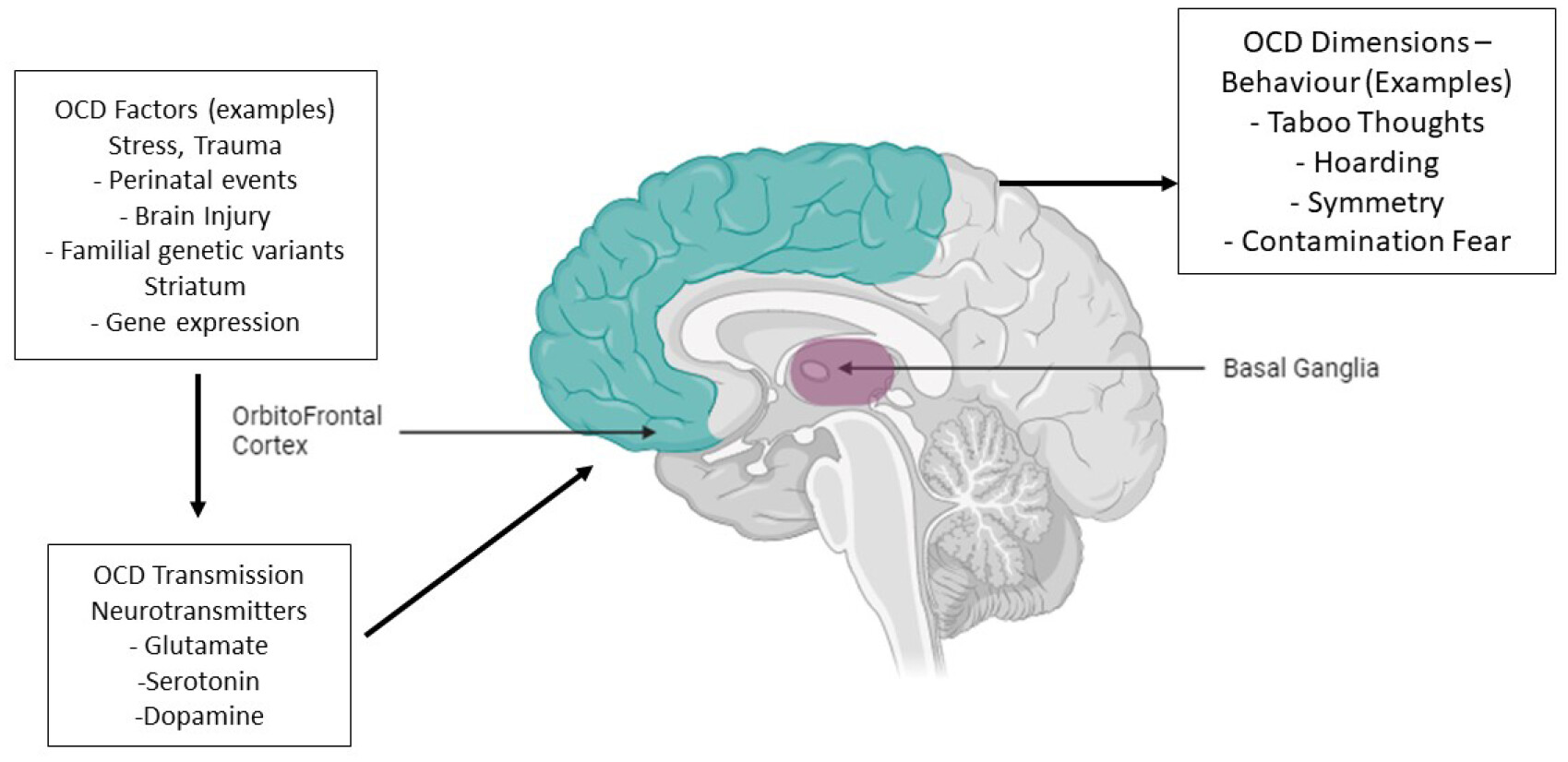
Human studies have confirmed these findings, linking early-life stressors and recent traumatic events to grey matter loss in corticostriatal-limbic circuitry, particularly in the medial prefrontal cortex (mPFC), anterior cingulate cortex (ACC), and orbitofrontal cortex (OFC) [16, 17]. These changes in brain structure and function are closely related to the anatomical substrates of habitual and goal-directed behavioural control, providing a neurobiological framework for understanding the impact of stress on OCD symptomatology [18, 19].
Five distinct mechanisms have been proposed to elucidate how stress may contribute to a bias toward habit formation and exacerbate OCD symptoms. Firstly, excessive stress can lead to atrophy of the caudate nucleus, impairing goal-directed control of behavior [20]. Conversely, stress-induced hypertrophy of the putamen may enhance sensorimotor habit formation, potentially perpetuating compulsive behaviors. Furthermore, stress-related impairment of complex spatial learning and memory processes, mediated by hippocampal dysfunction, may promote reliance on habitual responses. Additionally, stress-induced atrophy of the frontal cortices, particularly the mPFC and OFC, may disrupt goal-directed behavioral control and flexible switching between habitual and goal-directed systems. Finally, acute and prolonged stress may influence the balance between habit and goal-directed action through amygdala hyperactivity and hypertrophy over time.
It is critical to recognise that the specific effects of stress on an individual are likely influenced by a complex interplay between underlying vulnerability factors, such as genetic predispositions, and the nature, intensity, and duration of the stressful experience [15, 21]. Furthermore, excessive stress is likely to exert interactive effects across various anatomical regions, constituting an interconnected circuitry that eventually biases the brain toward rigid, habitual patterns of behaviour.
4 Interaction Between Genes and Environment in OCD
Understanding the genetic landscape of obsessive-compulsive disorder (OCD) is similar to navigating a complex maze in which genetic and environmental factors intersect to shape the manifestation of this debilitating condition [22, 23]. Family and twin studies have laid a strong foundation, revealing a heritable component in OCD, with afflicted individuals showing significantly higher rates of the disorder among their relatives than unaffected controls [24, 25]. This familial clustering suggests a genetic predisposition to OCD, prompting researchers to investigate the disorder's molecular underpinnings. Modern genomic techniques, such as genome-wide association studies (GWAS) and whole-exome sequencing, have revealed the complex genetic architecture of OCD [18, 24]. These studies suggest that OCD is not governed by a single gene, but rather by the cumulative effects of numerous genetic variants, each exerting a subtle influence on the disorder's predisposition [25]. While the majority of these variants are common and have minimal individual impact, there is emerging evidence indicating that rare genetic mutations may also play a role in certain individuals or families [26, 27].
Visualizing OCD's genetic landscape reveals a spectrum of risk, with some individuals harbouring few risk alleles, others carrying a multitude, and the majority falling somewhere in between [14]. This nuanced distribution highlights the polygenic nature of OCD, where the interplay of numerous genetic factors contributes to disease susceptibility [22, 25]. Despite significant advances in genomic research, identifying specific genetic changes remains elusive, with genome-wide association studies failing to identify individual genes or single-nucleotide polymorphisms (SNPs) with strong associations.
Nonetheless, candidate gene studies have implicated several genes in critical biological pathways relevant to OCD pathology [28, 29].
Genes involved in cytoskeleton dynamics, ion channel differentiation, and glutamatergic signalling have emerged as potential contributors to OCD. Furthermore, genes involved in glutamatergic neurotransmission and neuronal differentiation have received attention for their potential roles in OCD pathogenesis [30]. Population-based studies have further enriched our understanding of the genetic basis of OCD by unveiling associations between specific genetic loci and variations in obsessive-compulsive symptoms [31]. Notably, genes on the chromosomal region 19p13.11 have been implicated in modulating OCD-related behaviours, shedding light on the disorder's nuanced genetic landscape [31]. Interestingly, recent studies have broadened our view beyond common genetic variants, highlighting the potential contributions of rare genetic mutations and non-coding DNA to OCD aetiology [15,16, 22]. Rare coding mutations and changes in non-coding DNA, especially those affecting chromatin structure and histone modifications, may disrupt neurotransmitter systems involved in OCD pathophysiology [25]. Furthermore, gene-environment interactions have emerged as important players, influencing epigenetic signalling and neurotransmitter function in individuals predisposed to OCD [23, 30].
OCD's genetic landscape consists of common and rare genetic variants that are intertwined with environmental influences and epigenetic modifications. As researchers continue to unravel the complexities of OCD genetics, efforts to increase sample sizes, incorporate diverse populations, and explore novel genetic methodologies will be crucial [28, 31]. Only by fully understanding the genetic architecture of OCD can we hope to develop more effective treatments and interventions for this complicated disorder.
Halvorsen et al. (2021) [32] conducted a study on uncommon genetic variations and found persuasive evidence for their role in OCD pathophysiology. The researchers used whole-exome sequencing to identify uncommon coding variants related with OCD in a subgroup of people and families. These rare variations, despite their rarity, had significant effects on OCD development, offering light on the intricate interplay between common and rare genetic variables in the disorder's aetiology [32].
In a parallel line of investigation, Lin et al. (2022) [26] investigated the epigenetic landscape of OCD, revealing the complex involvement of chromatin changes in illness susceptibility. In a small-scale whole-genome sequencing analysis, the researchers discovered abnormal chromatin changes linked to OCD and similar illnesses. Mutations in promoter-anchored chromatin loops and areas with elevated histone marks were associated in OCD heredity, providing unique insights into the epigenetic mechanisms underlying the condition [26]. These ground-breaking findings highlight the multidimensional nature of OCD pathogenesis, in which genetic, epigenetic, and environmental variables interact to influence disease vulnerability and treatment response. Such research attempts pave the way for more tailored and effective approaches to OCD assessment and rehabilitation by clarifying the complicated interaction between hereditary and environmental effects.
5 Neurological Circuitry of OCD
Obsessive-compulsive disorder (OCD) is a multifaceted mental health condition distinguished by intrusive thoughts (obsessions) and repetitive behaviours or mental acts (compulsions) performed in response to these thoughts. Despite extensive research, the precise exact cause of OCD remains uncertain, prompting investigations into the complex neurocircuitry that underpins this debilitating disorder. At the forefront of these activities is the corticostriatal-thalamocortical (CSTC) circuitry, a complex neural network involved in a variety of cognitive and affective functions. Navigating the human brain's convoluted pathways, researchers discovered compelling evidence linking specific brain regions and their connectivity patterns to the pathophysiology of OCD.
Within the wide landscape of the human brain, the medial frontal cortex (mFC) emerges as a focus of interest in OCD research. Neuroimaging studies during symptom provocation have shown that the anterior cingulate cortex (ACC) and orbitofrontal cortex (OFC) are particularly hyperactive [29]. These findings emphasise the mFC's critical role in OCD pathology, specifically its involvement in the generation and regulation of obsessive-compulsive symptoms. Further investigation of the neuroanatomical substrates of OCD reveals changes in grey matter volumes in key brain regions, particularly the striatum (Figure 2). OCD patients show increased grey matter volume in the dorsal striatum, particularly the putamen, and decreases in the mFC, including the ACC [26]. These structural abnormalities indicate a dysregulated interaction between brain regions involved in OCD pathology, providing important insights into the disorder's neurobiological underpinnings.
Furthermore, studies of functional connectivity within the CSTC circuitry have revealed abnormal network dynamics in OCD. OCD patients exhibit increasing brain connectivity in the dorsal striatum and thalamus, as well as increased connectivity between the ventral striatum and the medial prefrontal cortex (mPFC) [33]. These findings emphasise the importance of network-level dysfunction in OCD pathogenesis, as well as the interconnectedness of brain regions involved in the disorder. In preclinical studies, altered activity within CSTC circuits was linked to the advancement of repetitive behaviours similar to OCD. Elevated activity in both the ventral and dorsal striatum serves as a precursor to compulsive grooming behaviours, shedding light on the neural substrates that underlies OCD symptoms [26]. Furthermore, stress-induced changes within CSTC circuits, such as dendritic atrophy and molecular alterations, shed light on the mechanistic underpinnings of OCD pathology, paving the way for new therapeutic interventions. The study of habit learning and expression reveals a fundamental difference between habitual and goal-directed behaviours in OCD. Individuals with OCD exhibit a preference for rigid habits, which reflects dysfunction in the dorsolateral and dorsomedial striatum, as well as changes in orbitofrontal cortex (OFC) activity. Moreover, dysregulation within structures implicated in fear and anxiety, such as amygdala hyperresponsivity and aberrant hippocampal activation, further contributes to the manifestation of habitual behaviors characteristic of OCD.
OCD's neurocircuitry is a complex interplay of neural networks that perform various cognitive and affective functions. From the bustling corridors of the medial frontal cortex to the intricate pathways of the striatum and beyond, the CSTC circuitry serves as a focal point for understanding the neurobiological underpinnings of OCD. Researchers hope that by elucidating the dynamic interplay between brain regions implicated in the disorder, they will pave the way for novel therapeutic interventions to alleviate the burden of OCD.
6 Clinical OCD pathogenesis and proposed mechanisms
Obsessive-compulsive disorder (OCD) is still unknown, with a complex pathogenesis woven from genetic, epigenetic, and environmental threads. OCD which is one such disorder through a complex interplay of factors, alluring both researchers and clinicians with its enigmatic origins.
At the heart of OCD is a genetic blueprint that guides its development with thorough precision. Twin studies have revealed a stark contrast between monozygotic and dizygotic pairs, with the former having a significantly higher concordance rate [34]. The familial clustering of OCD highlights its genetic basis, with first-degree relatives bearing a heavier burden of the condition [17]. Indeed, genetics has a significant impact on OCD symptoms, accounting for a large portion of the variability observed, particularly in children. In adults, genetic factors continue to have an impact, accounting for a sizable proportion of obsessive-compulsive symptoms. Furthermore, genes associated with the serotonergic and glutamatergic pathways may hold the key to understanding treatment response, offering a bit of hope for personalised therapeutic interventions [35,36, 37]. However, genes do not paint the entire picture; environmental factors add complex brushstrokes to the canvas of OCD pathogenesis. Stress, like a relentless tide, can shape the contours of OCD symptomatology, with many individuals reporting the onset of symptoms during periods of high stress [31, 35]. Childhood-onset OCD appears to be especially vulnerable to the effects of stress, though the precise nature of this relationship remains unknown. Nevertheless, the impact of stress on OCD cannot be underestimated, with studies suggesting a link between early life stress or trauma and the emergence of psychiatric symptoms [38, 39]. Furthermore, acute brain trauma, while less common, can cast a long shadow over OCD pathogenesis, complicating the complex web of causality.
As we investigate the complexities of OCD, it becomes clear that genetic risk factors transcend specific disorders, contributing to a shared vulnerability across neuropsychiatric conditions. The Brainstorm Consortium's groundbreaking research sheds light on this interconnectedness, revealing a high degree of genetic correlation among various disorders, including OCD [37]. This genetic overlap obscures the distinctions between conditions, emphasising the need for a comprehensive approach to understanding neuropsychiatric disorders. Recent advancements in whole-genome sequencing further illuminate this interconnectedness, highlighting a strong genetic overlap between OCD and Tourette syndrome [28].
OCD pathogenesis emerges as a complex symphony of genes, environment, and epigenetics, with each note adding to the rich tapestry of neuropsychiatric disorders. As we continue our quest for understanding, let us approach the complexity of OCD with humility and curiosity, knowing that its enigmatic depths hold the potential for profound discovery. As we delve deeper into the labyrinth of OCD pathogenesis, epigenetic modifications emerge as a silent but powerful force, shaping the neurobiological landscape with exquisite precision. Epigenetics, the study of heritable changes in gene expression that occur without alterations to the DNA sequence, provides a subtle view of the relationship between nature and nurture in OCD. Epigenetic mechanisms shape the expression of genes involved in OCD, shaping the neurobiological landscape in response to environmental cues [23]. DNA methylation, histone modifications, and non-coding RNAs play a delicate role in gene regulation, influencing neuronal function and synaptic plasticity. These epigenetic mechanisms encode the effects of genetic predispositions and environmental exposures into the brain's molecular architecture, shaping the trajectory of OCD development and progression. Studies on the epigenetic basis of OCD have yielded fascinating insights into the molecular mechanisms that underpin the disorder. Alterations in DNA methylation patterns at specific gene loci have been linked to the development of OCD, providing insight into the disorder's dysregulated gene expression profiles. Histone modifications, including acetylation, methylation, and phosphorylation, exert dynamic control over chromatin structure and gene transcription, influencing the expression of genes critical to OCD pathophysiology. Furthermore, non-coding RNAs, such as microRNAs, are emerging as key players in fine-tuning gene expression networks associated with OCD, adding to the epigenetic landscape's complexity.
Gene-environment interactions shape the epigenetic landscape of OCD, influencing susceptibility to the disorder and its progression. Early-life experiences, including exposure to stress, trauma, and adversity, can induce long-term epigenetic changes that predispose individuals to OCD later in life [25, 27]. These epigenetic imprints encode memories of prior experiences into the molecular fabric of the brain, perpetuating dysfunctional neural circuits associated with OCD symptoms [36].
In addition to environmental influences, pharmacological interventions used to treat OCD may have therapeutic effects via epigenetic mechanisms. Medications targeting serotonergic and glutamatergic pathways, such as selective serotonin reuptake inhibitors (SSRIs) and N-methyl-D-aspartate (NMDA) receptor modulators, have been shown to influence epigenetic processes, thus altering gene expression patterns and restoring neurobiological homeostasis [13,26, 40]. These medications, which target epigenetic mechanisms underlying OCD pathophysiology, provide a glimpse into the potential for precision medicine approaches tailored to individual patients' unique epigenetic profiles.
Despite progress in understanding the epigenetic underpinnings of OCD, many questions remain unanswered. The dynamic nature of epigenetic regulation complicates determining causal relationships between epigenetic modifications and OCD phenotypes. Longitudinal studies tracking epigenetic changes over time are required to better understand the temporal dynamics of epigenetic changes in OCD development and progression. Furthermore, the tissue-specificity of epigenetic modifications raises concerns about the relationship of peripheral biomarkers to central nervous system mechanisms underlying OCD pathophysiology.
7 Treatment Approaches of Obsessive-Compulsive Disorder
As our understanding of obsessive-compulsive disorder (OCD) has expanded, so have the treatment approaches for alleviating the distress and dysfunction associated with this debilitating condition. Historically, psychoanalytic and psychodynamic theories dominated the landscape of OCD treatment, but their efficacy was limited, prompting a shift toward more empirically supported approaches. Early attempts at behavioural therapy, such as systematic desensitisation and aversion therapy, produced mixed results, emphasising the importance of more targeted and effective interventions (Table 1).
| Treatment Approach | Description | Examples |
|---|---|---|
| EX/RP | Direct confrontation with feared stimuli while preventing ritualistic responses. Utilizes in-vivo exposure, imaginal exposure, and ritual prevention. | Meyer's EX/RP therapy |
| CT DBT Schema Therapy VRET ACT Biofeedback Neurofeedback DBS Pharmacologica Therapies | Identifies and challenges maladaptive thought patterns contributing to OCD. Helps patients recognize irrationality of fears and reinterpret obsessions, leading to reduced anxiety and reliance on rituals. Combines cognitive-behavioral therapy, mindfulness, and acceptance-based strategies to address emotion dysregulation and impulse control problems. Provides a comprehensive approach to managing distressing emotions and behaviors. Integrates cognitive-behavioral techniques with attachment theory to target core beliefs underlying OCD symptoms. Addresses deep-seated cognitive patterns contributing to obsessive-compulsive behaviors. Uses immersive technology to simulate anxiety-inducing scenarios, providing a safe yet realistic setting for exposure and response prevention. Allows controlled confrontation of feared situations. Increases psychological flexibility by encouraging acceptance of unwanted thoughts and emotions while aligning actions with personal values. Focuses on accepting internal experiences rather than trying to change or eliminate them. Teaches patients to manage physiological responses to anxiety by providing real-time feedback on bodily functions. Enhances awareness and control over physical reactions to stressors. Utilizes real-time fMRI feedback to train patients to regulate specific brain regions involved in OCD. Offers a personalized and non-invasive approach to modulating brain activity. Involves surgical implantation of electrodes in specific brain regions implicated in OCD. Sends electrical impulses to regulate abnormal neural activity. l Utilizes medications to reduce OCD symptoms by targeting neurotransmitter imbalances in the brain. Often used in combination with psychological interventions for enhanced efficacy. | Challenging irrational thoughts, reinterpreting obsessions Mindfulness practices, acceptance-based strategies Addressing core beliefs, attachment theory Immersive VR simulations, exposure in virtual environments Mindfulness practices, values clarification Monitoring heart rate variability, regulating breathing patterns Training in brain modulation, real-time feedback on neural activity Surgical electrode implantation, electrical stimulation of brain regions SSRIs, dopamine agonists, glutamate modulators |
Meyer pioneered exposure and ritual prevention (EX/RP) therapy in 1966, which revolutionised OCD treatment. EX/RP represents a paradigm shift in OCD treatment, emphasising direct confrontation with feared stimuli while preventing ritualistic responses. Patients gradually learn to tolerate distressing thoughts and situations without engaging in compulsive behaviours through a combination of in-vivo exposure, imaginal exposure, and ritual prevention. Studies have consistently shown that EX/RP is effective at reducing OCD symptoms, with many patients maintaining their gains over time.
Additional research has attempted to determine the relative contributions of various components of EX/RP therapy. Imaginal exposure, in which patients vividly imagine distressing scenarios, has been shown to improve treatment outcome maintenance over time. Similarly, combining in-vivo exposure and ritual prevention has been shown to produce better results than either component alone. These findings highlight the importance of tailoring treatment approaches to individual patients' needs, incorporating a variety of exposure techniques to maximise therapeutic benefits.
In addition to EX/RP therapy, cognitive therapy (CT) has emerged as a promising method for treating OCD. CT seeks to identify and challenge maladaptive thought patterns that contribute to obsessive and compulsive behaviour. CT facilitates a shift in cognitive perspective by assisting patients in recognising the irrationality of their fears and reinterpreting the meaning of their obsessions, resulting in reduced anxiety and reliance on compulsive rituals. Studies comparing CT to EX/RP found that both approaches were equally effective in reducing OCD symptoms, emphasising the importance of providing patients with a variety of treatment options to meet their specific preferences and needs.
Recent meta-analyses have added to the evidence base for EX/RP and CT, demonstrating their efficacy in reducing OCD symptoms across a wide range of patient groups. Furthermore, these analyses have highlighted the importance of individual treatment planning, with therapy outcomes being influenced by factors such as treatment adherence, therapist competence, and patient motivation [41]. While EX/RP and CT are considered the gold standard in OCD treatment, pharmacotherapy remains an important component of management for many patients. Selective serotonin reuptake inhibitors (SSRIs) have been shown to effectively reduce OCD symptoms in a large number of patients, especially when combined with psychological interventions like EX/RP or CT. However, medication alone is frequently insufficient for achieving optimal results, highlighting the significance of combining pharmacological and psychological approaches in the treatment of OCD.
Future research should focus on improving existing treatment protocols and investigating novel interventions for OCD. Advances in technology, such as virtual reality exposure therapy, show promise for improving the efficacy and accessibility of exposure-based treatments. Furthermore, more attention should be paid to addressing treatment barriers and disparities, especially among underserved populations who may have difficulty accessing evidence-based care.
Among the innovative treatment options for obsessive-compulsive disorder (OCD), Dialectical Behavior Therapy (DBT) stands out for its effectiveness in addressing emotion dysregula-tion and impulse control problems [42, 43]. DBT combines cognitive-behavioral therapy, mindfulness, and acceptance-based strategies to provide patients with a comprehensive approach to managing distressing emotions and maladaptive behaviours. Group therapy also appears to be a valuable option, providing individuals with OCD a supportive environment to share experiences, learn coping skills, and combat feelings of isolation [44]. Schema Therapy, which combines cognitive-behavioral techniques with attachment theory, targets core beliefs that underpin OCD symptoms and has demonstrated promise in preliminary studies [45]. Virtual Reality Exposure Therapy (VRET) uses immersive technology to simulate anxiety-inducing scenarios, providing a safe but realistic setting for exposure and response prevention. Acceptance and Commitment Therapy (ACT) increases psychological flexibility by encouraging patients to accept unwanted thoughts and emotions while aligning their actions with personal values [46]. Biofeedback, a technique focusing on physiological regulation, may supplement traditional therapies by teaching patients to manage their physical responses to anxiety [47]. These emerging treatment modalities broaden the therapeutic toolkit for OCD, providing new options for symptom relief and improved quality of life.
In recent years, advances in neuroimaging techniques have paved the way for novel treatment options for OCD by providing insights into the disorder's underlying neural mechanisms. Functional magnetic resonance imaging (fMRI) has been useful in identifying abnormal brain activity patterns associated with OCD symptoms, thereby providing potential targets for intervention. Neurofeedback therapy is one treatment approach that takes advantage of fMRI findings. Neurofeedback uses real-time fMRI feedback to train people to regulate specific brain regions involved in OCD, such as the orbitofrontal cortex and anterior cingulate cortex [48]. Neurofeedback, which teaches patients to modulate their brain activity, holds promise as a personalised and non-invasive treatment for OCD.
Deep brain stimulation is another emerging treatment modality based on fMRI research (DBS). DBS is the surgical implantation of electrodes in specific brain regions implicated in OCD, such as the ventral capsule/ventral striatum (VC/VS) or the anterior limb of the internal capsule (ALIC). These electrodes send electrical impulses to regulate abnormal neural activity and alleviate OCD symptoms [49, 50]. fMRI-guided DBS enables precise targeting of dysfunctional brain circuits, increasing treatment efficacy while reducing side effects. Although still considered experimental, DBS has shown promising results in treatment-resistant OCD cases, providing hope for those who have not responded to traditional therapies.
In addition to fMRI-guided interventions, other brain imaging techniques have the potential to improve OCD treatment outcomes. Positron emission tomography (PET) imaging, for example, allows for the assessment of neurotransmitter function in the brain, which provides important insights into the neurochemical basis of OCD. PET studies have implicated abnormalities in serotonin, dopamine, and glutamate neurotransmission in OCD pathophysiology, indicating potential targets for pharmacological interventions [51]. Pharmacological therapies tailored to individual neurochemical profiles may provide personalised treatment options for OCD by targeting specific neurotransmitter systems [52].
Furthermore, diffusion tensor imaging (DTI) has revealed structural abnormalities in white matter tracts connecting various brain regions in OCD. DTI studies revealed altered integrity and connectivity in cortico-striatal-thalamo-cortical circuits, which are implicated in the generation of OCD symptoms [27, 53]. Targeting white matter abnormalities with interventions like transcranial magnetic stimulation (TMS) or transcranial direct current stimulation (tDCS) has the potential to modulate aberrant neural connectivity and mitigate OCD symptoms. The incorporation of neuroimaging techniques into OCD treatment paradigms opens up exciting possibilities for personalised and targeted interventions [54, 55]. Brain imaging holds the key to unlocking novel OCD treatment modalities, including fMRI-guided neurofeedback and DBS, PET-informed pharmacotherapy, and DTI-based neuromodulation. These cutting-edge approaches have the potential to revolutionise the management of OCD by elucidating the neural circuits underlying its pathophysiology, giving hope to those who suffer from its symptoms. As research in this field advances, the future looks promising for more effective, tailored, and innovative treatments for OCD.
8 Conclusion and Future Perspective
The extensive body of literature investigating the relationship between stress and obsessive-compulsive disorder (OCD) symptomatology provides valuable insights on the aetiology and maintenance of this complex disorder. However, despite the abundance of cross-sectional studies and retrospective reports discussed above, there is a significant gap in mechanistic research that directly investigates this relationship. To meet these challenges, future research should use quasi-experimental designs to test hypotheses about the role of stress in OCD symptomatology. One potential approach is to compare habit learning between OCD patients with and without a history of trauma. Researchers can learn more about how trauma affects the development and manifestation of OCD symptoms by investigating habit learning in these two groups. Furthermore, neuroimaging techniques can help us understand whether stress or trauma exacerbate abnormalities in corticostriatal-limbic circuits. Investigating these circuits at rest, during symptom provocation, or during habit and goal-directed control tests can provide important insights into the neurobiological mechanisms that underpin the stress-OCD relationship.
Despite the high prevalence of trauma in OCD and the routine assessment of trauma exposure during clinical screenings, there is a significant lack of preclinical research using stress-based models to elucidate the pathophysiology of the disorder. Preclinical models of fear conditioning and chronic stress have been useful in studying the neurobiology of other trauma-related disorders, providing important insights into how stress affects habitual fear-motivated behaviours. As a result, future preclinical studies on stress-based models of OCD can provide critical information about the neural mechanisms underlying stress-induced exacerbation of OCD symptoms.
Furthermore, it has been suggested that OCD symptoms are similar to displacement behaviours seen in animals, such as grooming, which is known to be affected by stress. Although much of this research has been conducted in preclinical models of Tourette's syndrome (TS), which has neurobiological correlates with OCD and is also exacerbated by stress, the findings highlight the potential of animal models to elucidate the effects of stress on the etiology and pathophysiology of OCD. Survey studies suggest that excessive stress may play a significant role in the aetiology and maintenance of OCD symptoms, but our understanding of the underlying mechanisms is limited. The proposed imbalance between goal-directed and habitual control of behaviour in OCD, as well as associated changes in limbic and corticostriatal circuitry, provides a promising framework for understanding how stress affects OCD. Future research should focus on investigating these mechanisms through both clinical and preclinical approaches.
Furthermore, the recent focus on the effect of stress on OCD at both the clinical and mechanistic levels emphasises the importance of continuing research in this area. Increasing our understanding of the relationship between stress and OCD will not only help us better understand the disorder's pathophysiology, but will also pave the way for the development of new treatment and prevention strategies. Continuing on the path of understanding the complex relationship between stress and OCD, more research is required to fully comprehend the multifaceted nature of this interaction. Future study aims to look into the role of genetic and epigenetic factors in mediating stress-induced OCD susceptibility and severity. Given the evidence pointing to a genetic component to OCD and the possibility of gene-environment interactions, research focusing on identifying specific genetic variants or epigenetic modifications that influence susceptibility to stress-induced exacerbation of OCD symptoms could provide invaluable information. Moreover, longitudinal studies are required to better understand the temporal dynamics of stress and OCD symptomatology. By tracking individuals over time, researchers can investigate how fluctuations in stress levels correspond to changes in OCD symptoms, shedding light on the causal relationship. Furthermore, longitudinal studies enable the identification of potential moderators and mediators that may influence the strength and direction of the stress-OCD relationship, such as coping mechanisms, social support, and personality traits. Moreover, the role of early life stress in shaping the developmental trajectory of OCD warrants closer examination. Childhood-onset OCD has been associated with heightened susceptibility to stress, but the underlying mechanisms remain poorly understood.
Longitudinal studies starting from infancy and childhood can provide insights into how early life stressors contribute to the emergence and persistence of OCD symptoms across the lifespan. Such research could inform early intervention strategies aimed at mitigating the impact of stressors and preventing the onset of OCD in vulnerable individuals.
Conversely, given the diversity of OCD presentations, future research should look into potential subtypes of OCD that are more sensitive to stress. Subtyping OCD based on symptom dimensions such as contamination/washing, symmetry/ordering, hoarding, and intrusive thoughts may reveal differences in vulnerability to stressors and inform personalised treatment approaches. Furthermore, looking into cultural and sociodemographic factors that influence stress and OCD symptoms can help us gain a better understanding of these complex phenomena across different populations.
Together with advanced neuroimaging techniques, such as functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI), in longitudinal and experimental studies can help to better understand the neural mechanisms underlying the strain relationship. Researchers can identify neural circuits involved in the exacerbation of OCD symptoms caused by stress by studying changes in brain structure and function in response to acute and chronic stressors. Furthermore, studies that use transcranial magnetic stimulation (TMS) and deep brain stimulation (DBS) can investigate the therapeutic potential of targeting specific brain regions involved in stress regulation and OCD pathophysiology.
Increasing our understanding of the complex interplay between stress and OCD necessitates a multifaceted approach that incorporates clinical, genetic, epigenetic, developmental, and neurobiological perspectives. By elucidating the mechanisms by which stress influences the onset, course, and severity of OCD symptoms, researchers can pave the way for the development of more effective interventions that address both stress reduction and OCD symptoms. Finally, such efforts have the potential to improve outcomes and quality of life for people with OCD.
Acknowledgments
Not applicable.
Ethics approval
Not applicable
Consent to participate
Not applicable
Declaration of conflicting interests
The authors declare no conflicts of interest
Funding information
Not applicable
Footnote
Authors' information Akshita Debnath is the corresponding author of the manuscript and Souhrid Sarkar is the co-author. Both the authors are affiliated to Amity University Kolkata.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
References
1. Ruscio AM, Stein DJ, Chiu WT, et al. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry 2010, 15(1): 53-63. mp.2008.94.
2. Huppert JD, Franklin ME. Cognitive behavioral therapy for obsessive-compulsive disorder: an update. Curr Psychiatry Rep 2005, 7(4): 268-273.
3. Abramowitz JS. Comorbidity in obsessive-compulsive disorder. J Lifelong Learn Psychiatry 2019, 17(1): 509-520.
4. Ruscio A, Khalsa S, Perez Benitez CI, et al. Barriers to diagnosis and treatment of obsessive-compulsive and related disorders in low-and middle-income countries. BJPsych Open 2018, 4(6): 491-496.
5. Boals A. Trauma in the eye of the beholder: objective and subjective definitions of trauma. J Psychother Integr 2018, 28(1): 77-89.
6. Larsen SE, Pacella ML. Comprehensive concept-tualization and treatment of comorbid obsessive-compulsive disorder and major depressive disorder. Clin Psychol (New York) 2016, 23(1): 30-43.
7. Association AP. Diagnostic and Statistical Manual of Mental Disorders[M]. American Psychiatric Association, 2013.
8. Fontenelle LF, Miguel EC, Ferrao YA, et al. Onset of obsessive-compulsive disorder in childhood and adolescence: relation to stressful life events. Soc Psychiatry Psychiatr Epidemiol 2021, 56(10): 1791-1798.
9. Arnold PD, Banca P, Vaghi MM. Inoculation against learned OCD-like fear but not anxiety sensitivity requires inhibition of BLA microcircuits. Nat Commun. 2020, 11(1): 1-17.
10. Pittenger C, Kelmendi B, Wasylink S, et al. Riluzole augmentation in treatment-refractory obsessive-compulsive disorder: a series of 13 cases, with long-term follow-up. J Clin Psychopharmacol 2008, 28(3): 363-367.
11. Taylor S, Abramowitz JS. Interpersonal sensitivity and obsessive-compulsive symptoms: The mediating role of inferential confusion. J Anxiety Disord. 2012; 26(4):495-503.
12. Schwabe L, Wolf OT. Learning under stress impairs memory formation. Neurobiol Learn Mem 2010, 93(2): 183-188.
13. Dias-Ferreira E, Sousa JC, Melo I, et al. Chronic stress causes frontostriatal reorganization and affects decision-making. Science 2009, 325(5940): 621-625.
14. Dias-Ferreira E, Vieira JB, Mesquita AR, et al. Cortical-striatal BDNF processing underlies stress-enhanced habit formation. PLoS One 2012, 7(12): e52186.
15. Gillan CM, Papmeyer M, Morein-Zamir S, et al. Disruption in the balance between goal-directed behavior and habit learning in obsessive-compulsive disorder. Am J Psychiatry 2011, 168(7): 718-726.
16. Teicher MH, Anderson CM, Ohashi K, et al. Differential effects of childhood neglect and abuse during sensitive exposure periods on male and female hippocampus. Neuroimage 2018, 169: 443-452.
17. McEwen BS, Bowles NP, Gray JD, et al. Mechanisms of stress in the brain. Nat Neurosci 2015, 18(10): 1353-1363.
18. Graybiel AM. Habits, rituals, and the evaluative brain. Annu Rev Neurosci 2008, 31: 359-387.
19. Arnsten AFT. Stress signalling pathways that impair prefrontal cortex structure and function. Nat Rev Neurosci 2009, 10(6): 410-422.
20. Arnsten AFT. Stress weakens prefrontal networks: molecular insults to higher cognition. Nat Neurosci 2015, 18(10): 1376-1385.
21. Pauls DL. The genetics of obsessive-compulsive disorder: a review. Dialogues Clin Neurosci 2010, 12(2): 149-163.
22. Purty A, Antony A, Leslie CA, et al. Research for clinicians section: genetic contribution in obsessive-compulsive disorder—a comprehensive exploration. Indian J Psychiatry. 2019;61(Suppl 1):S90.
23. Stewart SE, Yu D, Scharf JM, et al. Genome-wide association study of obsessive-compulsive disorder. Mol Psychiatry 2013, 18(7): 788-798.
24. Mattheisen M, Samuels JF, Wang Y, et al. Genome-wide association study in obsessive-compulsive disorder: results from the OCGAS. Mol Psychiatry 2015, 20(3): 337-344.
25. den Braber A, Zilhao NR, Fedko IO, et al. Obsessive-compulsive symptoms in a large population-based twin-family sample are predicted by clinically based polygenic scores and by genome-wide SNPs. Transl Psychiatry 2016, 6(2): e731.
26. Cappi C, Brentani H, Lima L, et al. Whole-exome sequencing in obsessive-compulsive disorder identifies rare mutations in immunological and neurodevelopmental pathways. Transl Psychiatry 2016, 6(3): e764.
27. Cappi C, Azevedo MH, Rozenthal D, et al. Rare copy number variants in early-onset OCD: another piece of the puzzle. J Am Acad Child Adolesc Psychiatry 2020, 59(11): 1249-1258.
28. Halvorsen M, Holmgren E, Arstad S, et al. Rare genetic variants related to glutamate and the encoding of prior experience in obsessive-compulsive disorder. Sci Rep 2021, 11: 15845.
29. Lin Z, Huang B, Su Q, et al. Epigenetic alterations in obsessive-compulsive disorder. Transl Psychiatry. 2022; 12(1):1-13.
30. Brennan BP, Rauch SL, Jensen JE, et al. A critical review of magnetic resonance spectroscopy studies of obsessive-compulsive disorder. Biol Psychiatry 2013, 73(1): 24-31.
31. Arnold PD, Reddy YC, Swedo SE. Research for clinicians: cellular and circuit mechanisms in obsessive-compulsive disorder. Focus (Am Psychiatr Publ) 2018, 16(1): 24-33.
32. Posner J, Marsh R, Maia TV, et al. Reduced functional connectivity within the limbic cortico-striato-thalamo-cortical loop in unmedicated adults with obsessive-compulsive disorder. Hum Brain Mapp 2014, 35(6): 2852-2860.
33. Jenike MA. Clinical practice. Obsessive-compulsive disorder. N Engl J Med 2004, 350(3): 259-265.
34. Brock H. Obsessive-compulsive disorder. StatPearls. 2023. Available at: https://www.ncbi.nlm.Nih.gov/books/NBK553162/ (accessed 29 May 2023).
35. Brandl EJ, Tiwari AK, Zhou X, et al. Influence of CYP2D6 and CYP2C19 gene variants on antidepressant response in obsessive-compulsive disorder. Pharmacogenomics J 2014, 14(2): 176-181.
36. Miguelez-Pan M, Ratia M, Meana JJ, et al. Different responses to chronic fluoxetine treatment in two inbred mice strains assessed in the forced swimming test: Parallels with OCD spectrum disorders and comorbid depression in the clinic. Psychopharmacology (Berl) 2011, 215(2): 353-362.
37. Qin N, Hu B, Xu L, et al. Genetic polymorphisms in the SLC6A4 gene expression in major depressive disorder and in antidepressant response. Medicine (Baltimore) 2016, 95(48). 10.1097/MD.0000000000005391.
38. Adams TG, Ford KL, Anderson GR, et al. Change in obsessive compulsive symptoms after experimental stress induction: Role of perceived control. J Anxiety Disord 2018, 57: 71-75.
39. Murphy ML, Slavny S, DePierro J. Life stress and pediatric obsessive compulsive disorder: The role of new daily stressors and sex in symptom exacerbation. Psychiatry Res. 2016;245:231-239.
40. Carpenter L, Chung MC. Childhood trauma in obsessive compulsive disorder: the roles of alexithymia and attachment. Psychol Psychother 2011, 84(4): 367-388.
41. Park SH, Joo YH, Lee JY, et al. Prevalence, correlates, and comorbidities of four DSM-IV specific obsessive-compulsive personality disorders in the Korean general population. J Psychiatr Res 2013, 209(3):596-603.
42. Brainstorm Consortium, Anttila V, Bulik-Sullivan B, et al. Analysis of shared heritability in common disorders of the brain. Science 2018, 360(6395): eaap8757.
43. Pittenger C., Kelmendi B., Bloch M., Krystal J. H., Coric V. (2005). Clinical treatment of obsessive compulsive disorder. Psychiatry (Edgmont (Pa. : Township)), 2(11), 34-43. 43. Pittenger C, Kelmendi B, Bloch M et al. Clinical treatment of obsessive compulsive disorder. Psychiatry (Edgmont) 2005, 2(11): 34-43.
44. Pauls DL, Abramovitch A, Rauch SL, et al. Obsessive-compulsive disorder: an integrative genetic and neurobiological perspective. Nat Rev Neurosci 2014, 15(6): 410-424.
45. Uhre V, Uhre C, Lenfeldt N, et al. P.873 Cognitive behavioral therapy for obsessive-compulsive disorder in children and adolescents, a systematic review with meta-analysis and trial sequential analysis. Z Kinder Jugendpsychiatr Psychother 2019, 46(1): 5-15.
46. Steketee G, Frost RO, Tolin DF. Diagnosis and assessment of obsessive-compulsive disorder. In: McKay D, Abramowitz JS, Taylor S, Asmundson GJG, eds. Current Directions in Obsessive-Compulsive Spectrum Disorders. Current Issues in the Treatment of Anxiety Disorders, vol 5. Springer; 2011.
47. Abramowitz JS, Baucom DH, Boeding S, et al. Treating obsessive-compulsive disorder in intimate relationships: a pilot study of couple-based cognitive-behavior therapy. Behav Ther 2013, 44(3): 395-407.
48. Frost RO, Tolin DF, Steketee G, et al. Cognitive behavioral therapy for hoarding disorder: Current status and future directions. J Obsessive Compuls Relat Disord. 2011;1(1):4-11.
49. Twohig MP, Hayes SC, Masuda A. Increasing willingness to experience obsessions: acceptance and commitment therapy as a treatment for obsessive-compulsive disorder. Behav Ther 2006, 37(1): 3-13.
50. Subramanian L, Hindle JV, Johnston S, et al. Real-time functional magnetic resonance imaging neurofeedback for treatment of Parkinson's disease. J Neurosci 2011, 31(45): 16309-16317.
51. Hampson M, Scheinost D, Qiu ML, et al. Biofeedback of real-time functional magnetic resonance imaging data from the supplementary motor area reduces functional connectivity to subcortical regions. Brain Connect 2011, 1(1): 91-98.
52. Greenberg BD, Malone DA, Friehs GM, et al. Three-year outcomes in deep brain stimulation for highly resistant obsessive-compulsive disorder. Neuropsychopharmacology 2006, 31(11): 2384-2393.
53. Vriend C, de Koning PP, Figee M, et al. Combined thalamic deep brain stimulation and nucleus accumbens shell stimulation for obsessive-compulsive disorder. Brain Stimul. 2018;11(1):190-193. s00701-016-3044-5.
54. Saxena S, Rauch SL. Functional neuroimaging and the neuroanatomy of obsessive-compulsive disorder. Psychiatr Clin North Am. 2000;23(3):563-586.
55. Fontenelle LF, Harrison BJ, Yucel M, et al. Neuroimaging and neuroimmunologic aspects of obsessive compulsive disorder. In: Costa DCL, ed. Obsessive Compulsive Disorder: Current Science and Clinical Practice. John Wiley & Sons; 2011:165-193.
Biographies

Souhrid Sarkar holds a BTech in Biotechnology from Department of Biotechnology, Amity University (2024). He is currently pursuing an MSc in Cancer Research and Precision Oncology at the University of Glasgow and associated as a Mentor at ASCO, with his sights set on a PhD focused on brain malignancies and neurological disorders. His interdisciplinary expertise is evidenced by his Springer publication, which explores the pivotal role of extracellular vesicles in neurodegenerative diseases and the intricate immunomodulatory signaling pathways in glioblastoma multiforme (GBM). Sarkar's pioneering work, recognized through prestigious Young Researcher Award, International Leadership Award, and India Merit Award, has significantly advanced the fields of cancer immunology and the development of novel immunotherapeutic strategies. With his deep insights into nanoparticle drug delivery systems and intercellular communication mechanisms, Sarkar's research trajectories hold immense promise for transforming patient outcomes in both neurological and oncological contexts. E-mail: [email protected]

Akshita Debnath received her BA (Hons) in Applied Psychology degree from the Department of Amity Institute of Psychology and Allied Sciences (2025), Amity University. Now she is a prospective MS and Ph.D. candidate. Her research focuses on exploring therapeutic applications of nanomedicine for stroke, trauma, and neurodegenerative disorders, with a particular emphasis on the psychological impacts and therapeutic approaches to improve patient's diagnosis. Debnath has authored the comprehensive review "Advancements in Nanoparticles for Drug Delivery, Therapeutic Applications and Computational Modeling," where she highlighted the potential psychological benefits of nanotherapeutics over conventional chemotherapy treatments. As a member of the British Psychological Society, her interdisciplinary work aims to develop psychologically-informed therapeutic interventions to enhance neurological outcomes and quality of life for patients. Email: [email protected]
Cite
Cite
Cite
OR
Download to reference manager
If you have citation software installed, you can download citation data to the citation manager of your choice
Information, rights and permissions
Information
Published In

Article first published online: June 22, 2024
Issue published: April-June 2024
Keywords
Rights and permissions
© The authors 2024.
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 License (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages (https://us.sagepub.com/en-us/nam/open-access-at-sage).
Request permissions for this article.
Data availability statement
Data is available for this article. View more information
Authors
Author contribution
Metrics and citations
Metrics
Publication usage*
Total views and downloads: 4593
*Publication usage tracking started in December 2016
Publications citing this one
Receive email alerts when this publication is cited
Web of Science: 0
Crossref: 5
- Post adversity changes in nigro-striatal dopamine: A mechanism for anxiety induced exacerbated innate repetitive behaviors
- From Stress to Obsession: The Role of Inferential Confusion and Obsessive Beliefs in Adolescent Obsessive‐Compulsive Symptoms
- Innovative treatment approaches for paediatric obsessive-compulsive disorder
- Scrupulosity in OCD and its association with religiosity and guilt – an exploratory study in Kashmir, North India
- Unraveling Gender Differences in Obsessive-Compulsive Disorder: A Focus on Key Micronutrients
Figures and tables
Figures & Media
Tables
View Options
View options
PDF/EPUB
View PDF/EPUBAccess options
If you have access to journal content via a personal subscription, university, library, employer or society, select from the options below:
I am signed in as:
View my profileSign out

I can access personal subscriptions, purchases, paired institutional access and free tools such as favourite journals, email alerts and saved searches.
loading institutional access options
Alternatively, view purchase options below:
Access journal content via a DeepDyve subscription or find out more about this option.
