1. Introduction
Sacroiliac joint (SIJ) dysfunction is considered to account for approximately 15%–30% of symptoms in patients with low back pain [
1–
3]. The SIJ is located between the sacrum and ilium and serves as a shock absorber that receives and aids in dissipating the impact of the trunk and lower limbs [
4,
5]. This joint is supported by tough ligaments and possesses low mobility compared to that of other synovial joints. Among the movements observed within the SIJ are nutation and counter-nutation, which are forward and backward rotations of the sacrum on the sagittal plane relative to the ilium, respectively. The SIJ is considered highly stable in the counter-nutation position [
6]. Unexpected force or repeated impact is believed to cause joint misalignment and instability and provoke pain arising from the SIJ [
7,
8]. Typical conservative (non-surgical) treatment strategies to relieve the painful SIJ include pelvic belts [
9,
10], injection of local anesthetics into the joint [
11,
12] and physical therapy [
6,
13]. Surgical treatment aims to fuse the SIJ, using metal implants [
14,
15]. Pelvic belts and SIJ fixations are used to improve joint stability by minimizing the extent of joint motion [
16,
17]. Some researchers have evaluated SIJ fixation using various implants [
14,
15] and the effects of such treatments on adjacent joints [
18,
19]. However, pelvic belts have not been comprehensively investigated in the context of SIJ dysfunction. A study in healthy young women indicated that pelvic belts help reduce SIJ laxity [
20]. Moreover, mathematical analysis indicates that compression force exerted on the anterior superior iliac spine (ASIS) increased SIJ compression and reduced muscle activity [
21]. These reports imply that if the SIJ is fixed with pelvic belts, stability would be enhanced, however, the effects based on the type and tightening method of the pelvic belts remain poorly understood. It has been reported that pelvic belts with a textured sacral pad may enhance the sensory performance of the hip joint and improve motor control [
22]. Compressive pelvic belts may also be beneficial in the treatment of SIJ dysfunction.
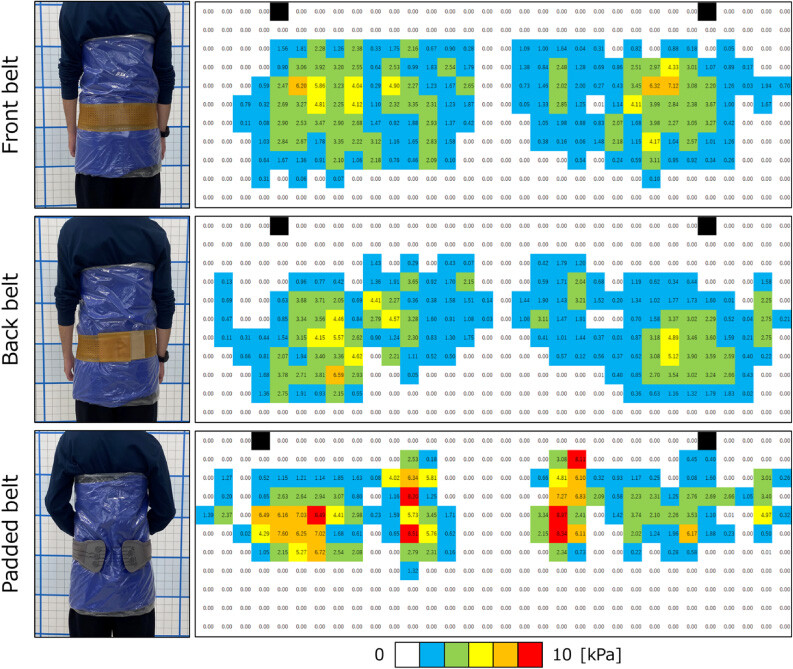
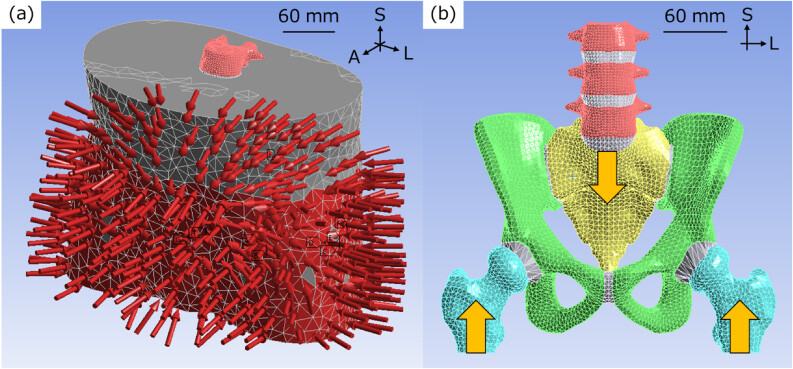
This study aimed to analyze the effect of pelvic rubber belts or padded pelvic belts on stress distribution within the pelvis and clarify the effectiveness of such treatments that bilaterally compress the posterior superior iliac spine (PSIS). The pressure distribution was assessed in the pelvic region when pelvic belts were applied. Finite element analysis of the pelvic model with soft tissues was conducted. It was hypothesized that padded pelvic belts would more effectively compress the SIJ and thus reduce tension of the surrounding ligaments.
4. Discussion
In this study, a rubber belt and a padded belt were investigated, showing similar load transfer mechanisms. Because the soft tissue is relatively thin in the anterior lateral parts of the lumbar region, the strain distribution on the pelvis matched the pressure point. Although the posterior pressure points were below the ASIS level, the pelvic area above the ASIS level was deformed. Regardless of the location of the pelvic belt, the upper part of the PSIS was compressed. The strain distribution in the pelvis with the padded belt was similar to that in the front and back belts, although the padded belt locally compressed the posterior region. This study suggests that the padded belt exerts the same pressure on the pelvis as the rubber belt, which may depend on the location of the pad. Statically, pressure on the buttocks reaches the upper part of the PSIS and compresses the posterior soft tissue, which is not considered to directly affect the pelvis. It may, however, support muscles and contribute to strengthening of the force closer [
32].
Pelvic belts are considered an established treatment for SIJ dysfunction. Bertuit et al. reported the effectiveness of pelvic belts in patients during pregnancy, where a visual analogue scale (VAS) at the SIJ was reduced by 20 mm in the group with a pelvic belt compared to the group without [
33]. Few studies, however, have investigated the mechanisms underlying treatment with pelvic belts in detail. In this study, the difference in the effect between the rubber belt and padded pelvic belt was investigated using finite element analysis.
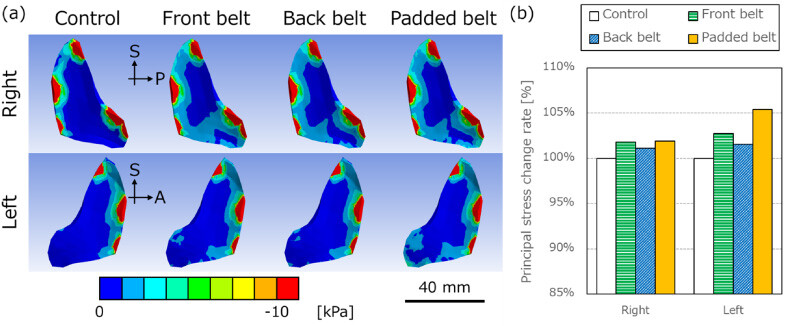
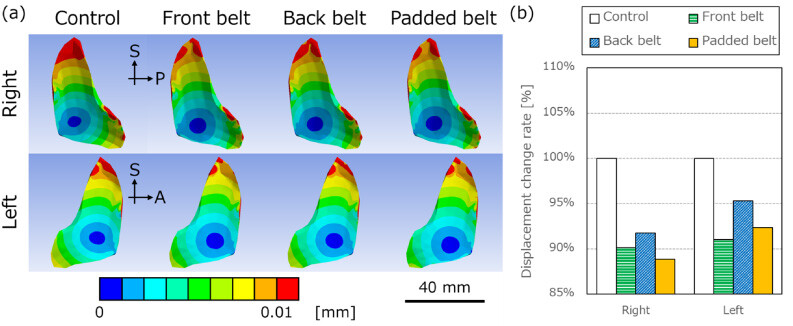
When the pelvic belt was applied, the displacement diagrams of the innominate bone showed that the anterior part of the bone moved outward, and the ischial limb was displaced inward, which indicated a relatively outward rotation of the innominate bone, called out-flare. The SIJs were considered to be in a compressed state because the compressive force increased, and the compressive stress area widened. Vleeming et al. reported that form and force closure improve SIJ stability, and the compressive force supports the force closure [
32]. Therefore, the pelvic belt reduced displacement of the SIJ and enhanced its stability.
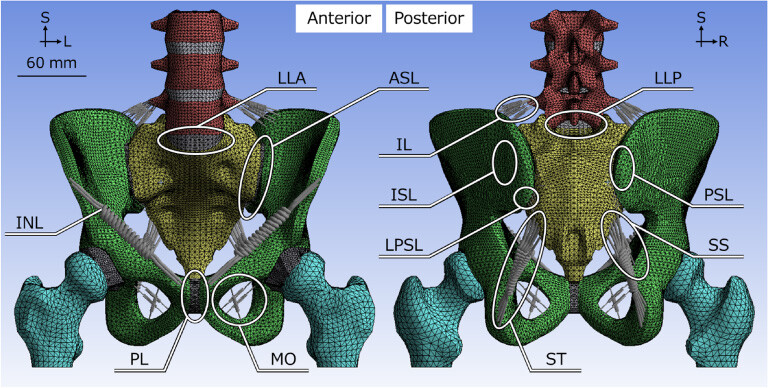
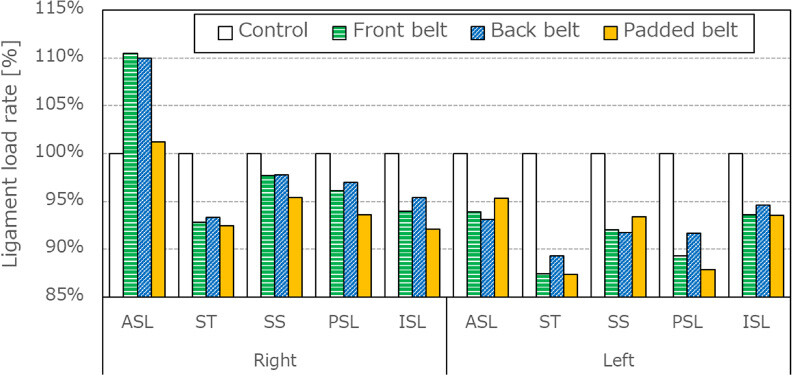
Ligament loading was reduced on the ST, SS, PSL and ISL. Sichting et al. [
31] also have reported that the mean strain values for the ST and SS decreased, which is consistent with the results of this study. The ST and SS are considered to limit the nutation motion [
34,
35], and pelvic belts seemed to weaken the nutation with subsequent ST and SS strains. The reduction in the loads of the PSL and ISL was caused by a decrease in SIJ displacement. The opposite loading trends of the ASL may have resulted from slight asymmetry of the pelvic belts or minute differences in the pressure exerted.
Klima et al. [
36] reported that the pelvic belt decreased the angles of nutation and increased the counter-nutation motion of the sacrum using human post-mortem tissues. Sichting et al. [
31] showed that the pelvic belt enhanced the inward rotation of the innominate bone on the coronal plane based on the measurement of the pelvis and SIJ deformation based on finite element analysis. These results differ from the outward rotation of the innominate bone on the transverse plane observed in this study. Sichting et al. [
31] placed the pelvic belt at a high position around the ASISs, which may be the reason that the results were different. This indicates that the height at which the pelvic belt is positioned may alter its therapeutic effects and treatment mechanisms. Depending on the position of the pelvic belts, patients with SIJ dysfunction reported increased pain relief despite using the same pelvic belts [
37]. Different patients and/or pathologies may require pelvic belts with different treatment mechanisms to reduce pain. In this study, all pelvic belts yielded similar effects on pelvic kinematics. Only the back belt exhibited a smaller decrease in displacement at the ASISs and SIJs than the others. The difference in the tightening pressure in each belt could have affected the results.
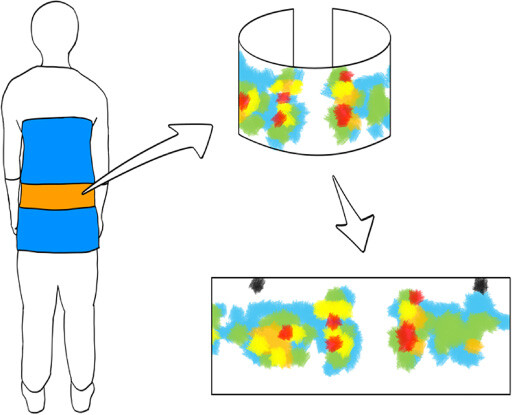
There are some limitations to this study. First, for simplification, the soft tissue was uniform in the model used in this study, and the role of the muscles was not considered. The soft tissue of the lumbopelvic region is mainly composed of skin, fat, and muscle, but these components were modeled as one soft tissue in this study. The material properties of each tissue are different, and muscle properties can change during standing and walking. In this actual measurement, the pressure distribution was different when the muscle worked, and the simulation should include the muscle conditions. Since these considerations are complicated and this study was conducted in a rest condition without any motion, a simple soft tissue setup was adopted. Second, the tension of the pelvic belt was not specifically controlled although the pelvic belts were worn as tightly as possible to minimize the tension difference in each belt. Third, the pressure distribution measurement system of the pelvic belt did not precisely follow the body shape. The device used in this study was mainly developed to measure body pressure distribution with the participant in the lying position. Because of its mat shape, it became columnar when wrapped around the body and could not be tracked in the exact position. In addition, this could affect the wearing condition of the pelvic belt, since it is necessary to attach the belt while maintaining the shape of the device. For future research, it is important to develop a measuring instrument that can track the shape of the lumbar region without interfering with the pelvic belt.