Trends in U.S. life expectancy have been worrisome for decades, but declines in life expectancy during the COVID-19 pandemic were drastic. Between 2019 and 2021, life expectancy declined from 78.8 years to 76.1 years, a drop of 2.7 years (
Arias et al. 2022;
Arias and Xu 2022). Most of the decline was due to COVID-19 and unintentional injuries, predominantly drug poisonings. Among the two causes of death contributing most to the decline in life expectancy between 2019 and 2020, COVID-19 contributed 61.2%, and unintentional injuries contributed 11.7% (
Arias and Xu 2022). Between 2020 and 2021, those percentages were 50.0% and 15.9%, respectively (
Arias et al. 2022). Drug poisoning mortality rates were high before the pandemic, particularly among working-age adults, but surged during 2020 and 2021, claiming nearly 200,000 lives (
National Institute on Drug Abuse 2023).
Prior to the pandemic, all-cause mortality rates varied considerably among U.S. counties. Counties with higher mortality rates had higher prevalence of behavioral and metabolic risk factors (e.g., smoking, obesity), poor physical and mental health, lower educational attainment and income, higher unemployment rates, and larger shares of some minoritized racial-ethnic groups (
Dobis et al. 2020;
Dwyer-Lindgren et al. 2017;
Graetz and Elo 2022;
McLaughlin and Stokes 2002). Likewise, prior to the pandemic, drug poisoning mortality rates were higher in counties with smaller shares of college-educated residents and higher poverty and unemployment rates (
Cano et al. 2023;
Monnat 2018,
2019;
Monnat et al. 2019) and in communities where large shares of residents reported poor mental health (
Kedia et al. 2020). Unlike with many other causes of death, prepandemic drug poisoning mortality was lower, on average, in counties with smaller shares of Black and Hispanic residents (
Zhu et al. 2022), although the racial distribution of drug poisoning deaths may have shifted during the pandemic (
Kariisa et al. 2022;
Monnat 2023).
Going into the pandemic, these place-level “preexisting conditions” meant that certain counties were more vulnerable than others to experiencing high COVID-19 mortality rates as well as high rates of drug poisoning and all-cause mortality. In terms of COVID-19 mortality, significantly higher mortality rates were observed in counties with smaller shares of college-educated adults, lower median household income, higher poverty and unemployment rates, higher prevalence of preexisting health conditions, and larger shares of Black and Hispanic populations in the early waves of the pandemic but larger White population shares in later waves (
Albrecht 2022;
Cheng, Sun, and Monnat 2020;
Jones et al. 2023;
Madlock-Brown et al. 2022). Using a machine-learning approach to evaluate 53 county-level contexts, one analysis found that counties’ racial-ethnic composition, education levels, median household income, and poverty rates were the strongest predictors of COVID-19 mortality rates (
Itzhak et al. 2022). Regarding all-cause mortality,
Stokes et al. (2021) found that rates of excess deaths from January 2020 to March 2021 were higher in counties with lower median income and education and with worse health profiles.
In general, such ecological studies examined a snapshot of time and provided few insights into whether the associations between county contexts and mortality evolved during the pandemic. A few studies examined how county predictors of COVID-19 deaths fluctuated during the early months of the pandemic. One tracked COVID-19 deaths for six months following each county’s first experience with COVID-19, finding that the county contexts that mattered varied based on how long COVID-19 was present in a county (
Madlock-Brown et al. 2022). A study of January through May 2020 found that the association between counties’ socioeconomic status (SES) and COVID-19 mortality flipped from positive to negative (
Clouston, Natale, and Link 2021). A study of April through November 2020 found that the importance of county education, income, and racial-ethnic composition for predicting COVID-19 mortality fluctuated over time (
Itzhak et al. 2022). During the early months of the pandemic, counties with larger shares of Black residents had higher COVID-19 mortality than did counties with larger shares of White residents, but this disparity disappeared in early 2021 and reversed in late 2021 (Bergmann, Ahlgren, and Stone 2022). Between the initial and Omicron waves, disparities in COVID-19 mortality between non-Hispanic White and Black adults shrank due to rising mortality among the former, declining mortality among the latter, and a growing mortality disadvantage in nonmetropolitan areas (
Lundberg et al. 2023).
These temporal analyses raise intriguing questions, which this study aims to answer. For instance, how did the importance of county contexts for county mortality fluctuate for not only COVID-19 mortality but also for drug poisoning mortality—a primary contributor to the decline in life expectancy during 2020 and 2021—and for all-cause mortality? The temporal analyses also raise questions about how the fluctuation in county-level predictors of drug poisoning and all-cause mortality during the pandemic compared to that before the pandemic. In other words, does the importance of county contexts for mortality typically fluctuate over time, or was the fluctuation during the pandemic atypical? Were certain county characteristics, such as socioeconomic and racial-ethnic composition and counties’ population health profiles, more important for predicting mortality during the pandemic than before the pandemic, as is sometimes implied in scholarly work and media coverage? There is reason to question this assumption. For instance, using European data,
Nielsen et al. (2021) concluded that the hyped sex differences in excess deaths during the pandemic were not unusual once put in temporal context.
Also unclear is how the importance of county contexts compares to that of states’ pandemic policies for predicting county deaths. Many states enacted containment policies, such as stay-at-home orders, to mitigate the spread of the virus, and economic support policies, such as rent moratoria, to counter the economic fallout. These policies affected health and mortality in complex ways (e.g.,
Boen et al. n.d.;
Kaslow et al. 2023;
Monnat et al. 2023;
Wolf et al. 2024). For instance, containment policies like mask mandates reduced COVID-19 mortality (
Hansen and Mano 2023), whereas containment policies like business closures increased mental health problems (
Monnat et al. 2023) and drug poisoning deaths (
Wolf et al. 2024). States’ bans on foreclosures and evictions reduced drug poisoning deaths (
Wolf et al. 2024) and buffered the impact of economic precarity on mental health (
Boen et al. n.d.) and COVID-19 death rates (
Sun and Bisesti 2023).
Social History of Disease Framework
Our study is informed by the SHDF, which puts cause-specific mortality in temporal context to better understand how and why social inequalities in it change over time (
Clouston et al. 2016). It hypothesizes four stages through which cause-specific mortality progresses in a population. Each stage has implications for social inequalities in diseases and their mortality risks. The first stage, “natural mortality,” captures the period in which there is little knowledge in the population about how to prevent or treat a disease and its mortality risk. Social inequalities in mortality may or may not exist in this stage. As knowledge emerges, it is unequally diffused across the population, ushering in the second stage, “producing inequalities.” Inequalities emerge because some individuals and communities have social, economic, and other structural advantages that facilitate access to lifesaving knowledge and technology. The third stage, “reducing inequalities,” occurs when knowledge about and technology for preventing and treating a disease and its mortality risks diffuse throughout the population. Success in the third stage can lead to the final stage, “reduced mortality and/or disease elimination.” Importantly, the framework also asserts that human interventions—for example, technology, medicine, or policies—can affect the duration of each stage and the magnitude and direction of the inequalities within each stage.
The SHDF is closely related to another framework for understanding health inequalities—fundamental cause theory (FCT). In its original conceptualization, FCT helps explain why the association between SES and health emerges and persists over time despite changes in epidemiologic environments and the mechanisms that connect SES to health (
Link and Phelan 1995;
Phelan, Link, and Tehranifar 2010). It asserts that individuals and communities with higher SES deploy their SES-related resources (e.g., money, power, knowledge, social connections) to obtain protective factors and avoid harmful factors regardless of the environment or mechanisms at play (
Clouston et al. 2016). FCT has been extended to understand other how other social disadvantages, including racism (
Phelan and Link 2015) and stigma (
Hatzenbuehler, Phelan, and Link 2013), affect health. The SHDF further asserts that the importance of social (dis)advantages for cause-specific mortality must be placed in temporal and spatial context. For example,
Clouston et al. (2016) used county-level data from 1969 to 2009 to show how the importance of county SES for predicting mortality from four causes of death differed across stages of the framework.
We propose that the SHDF has utility for conceptualizing how social inequalities in mortality evolved during the pandemic not just for COVID-19 deaths but also for drug poisoning and all-cause mortality. Based on the original application of the framework that analyzed county SES and cause-specific mortality (
Clouston et al. 2016), we posit that the importance of county SES for cause-specific mortality may have changed during the exogenous shock of the pandemic. Studies of COVID-19 deaths early in the pandemic support this speculation (
Clouston et al. 2021;
Kamis et al. 2021). However, the framework’s potential for understanding social inequalities in mortality during the pandemic extends beyond place-level SES to other place-level markers of (dis)advantage, and it extends beyond COVID-19 mortality to drug poisoning and all-cause mortality. In the following, we describe these extensions for the current study.
Extending the Framework to the Current Study
To develop a fuller picture of how social inequalities in mortality fluctuated during the pandemic, we extend the framework in two ways. First, we examine all-cause mortality in addition to two causes of death of upmost importance during the pandemic, drug poisoning and COVID-19. All-cause mortality provides a complete picture, which may be distinct from that of any specific cause of death. For instance, place-level social inequalities in mortality from some causes may have widened but narrowed, persisted, or reversed for others (e.g.,
Miech et al. 2011), potentially leaving social inequalities in all-cause mortality unchanged. It is imperative to understand the net effect of these disparate trends and their implications for current and future mortality inequalities.
The second way that we propose extending the framework is to expand the scope of county-level (dis)advantages. In addition to SES and SES-related resources, we consider counties’ racial-ethnic composition and population health profiles. We posit that in the face of a shock like the pandemic, the importance of these factors for all-cause mortality, COVID-19 mortality, and drug poisoning may also change in systematic ways. Next, we describe some of these potential changes.
The association between county SES and mortality may have fluctuated for several reasons. Higher educated counties and those with higher median income may fare better on COVID-19 mortality if their residents can isolate by working from home and are able to avoid crowded stores by ordering food delivery (
Reeves and Rothwell 2020). Residents of counties with high-quality internet may have more opportunities for telehealth to diagnose and treat physical and mental health conditions (
Pandit et al. 2023). The comfort, resources, and control that higher income and education provide may also mean lower stress and anxiety—psychological hardships that increase risks of multiple causes of death. As an SES-related resource, health care infrastructure is also an important county-level resource. It may be more important in the face of a pandemic as demand for services increases.
In terms of county racial-ethnic composition, structural racism constrains access to flexible resources, like medical knowledge, power, and money, that are critically important during a pandemic (
Garcia et al. 2021;
Laster Pirtle 2020;
Phelan and Link 2015). In line with FCT’s argument that structural racism is a fundamental cause of health disparities, the importance of county racial-ethnic composition for mortality may have increased during the pandemic in part because Black and Hispanic individuals were more likely than White individuals to be working in essential industries and live in crowded housing (
Almagro et al. 2021;
DeLuca, Papageorge, and Kalish 2020), conditions that increase disease transmission.
A county’s population health profile is also a marker of (dis)advantage that affects access to resources and the diffusion of information and support. Adverse health behaviors, metabolic vulnerabilities, and poor physical and mental health, which are tied to SES, elevate mortality risk (
DeSalvo et al. 2006;
Masters et al. 2013;
Thun et al. 2013;
Yang et al. 2020). Counties with large shares of health-vulnerable populations had a high risk of COVID-19 deaths and consequently, of an overburdened health care system, reducing resources to treat other health conditions. By contrast, counties with favorable health profiles may have fared better if their health, as a community resource, lessened the severity of cases, keeping hospital beds open and physicians available for all health care needs of all residents. The importance of such resources for mortality may fluctuate during a pandemic. For example, the importance of a county’s population health profile may increase when there is no vaccine or effective treatment. The importance may increase when mobility restrictions and an overburdened health care system reduce access to routine health care, which may be most detrimental for counties with high shares of residents with poor mental and physical health. The importance of counties’ mental health may increase because people with poor mental health are less likely to have beneficial social connections (
Umberson and Montez 2010) through which helpful knowledge and resources related to the pandemic could be diffused. Indeed, in a study of another type of exogenous shock—Hurricane Katrina—
Raker, Zacher, and Lowe (2020) found that the stressors it imposed had the largest adverse effects among people with preexisting psychological distress and fair/poor health. Already high rates of social isolation among individuals with poor mental health likely increased during the pandemic due to social distancing protocols, elevating the risk for multiple causes of death. In sum, understanding how prepandemic county (dis)advantages predicted mortality during the unique conditions of the pandemic requires expanding the focus beyond SES resources to other place-level markers of (dis)advantage.
Figure 1, Panel A illustrates how the importance of county contexts for county COVID-19 mortality rates may fluctuate over time according to the SHDF. For heuristic purposes, we use county SES as the measure of (dis)advantage. The figure illustrates that prior to the pandemic, the risk of dying from COVID-19 was effectively zero (or undefined) in both advantaged and disadvantaged counties. At the start of the pandemic, COVID-19 mortality rises for both types of counties because there is little knowledge about disease spread and containment strategies have not yet been enacted (Stage 1). As knowledge about the disease and how to reduce its spread emerges (e.g., physical distancing), advantaged counties are better equipped to respond. The residents of these counties are more likely to be able to work remotely, live in uncrowded housing, have food and other supplies delivered to their homes, and more. As a result, county contexts become important predictors of COVID-19 mortality, and inequalities between advantaged and disadvantaged counties increase (Stage 2). As knowledge diffuses, vaccines are developed and widely disseminated, and pandemic mitigation policies are enacted, COVID-19 mortality declines for disadvantaged counties, and inequalities diminish (Stage 3). Eventually, COVID-19 inequalities shrink, and mortality approaches zero for both types of counties (Stage 4). Whether social inequalities in COVID-19-related deaths across counties followed these hypothesized stages is unclear, although evidence from the early months of the pandemic provides some support (
Clouston et al. 2021;
Kamis et al. 2021). Also unclear is whether other markers of county-level (dis)advantages discussed previously followed similar patterns.
Figure 1, Panel B shows a hypothetical example of how the importance of county contexts for drug poisoning deaths may have fluctuated. In this example, disadvantaged counties had consistently higher drug poisoning mortality than did advantaged counties before the pandemic (
Monnat 2018;
Monnat et al. 2019). At the start of the pandemic, the figure shows drug poisoning mortality rising in both types of counties. During this time, many states imposed stay-at-home orders and closed schools and nonessential businesses, and many health care providers (including mental health and substance use treatment providers) cancelled appointments or moved to telehealth (
Johnson et al. 2022). These institutional responses to the pandemic created novel and unrecognized threats across both advantaged and disadvantaged counties. States’ pandemic containment measures such as stay-at-home orders increased drug poisoning mortality (
Wolf et al. 2024) likely through social isolation (
Tull et al. 2020), disruptions to mental health and substance use treatment (
McNeely et al. 2021;
Mellis, Potenza, and Hulsey 2021), job loss (
Gupta et al. 2023), increases in solitary drug use (
Schneider et al. 2023), and more. Eventually, in this hypothetical example, drug poisoning mortality in advantaged counties starts declining toward its prepandemic level, thereby widening county inequalities. In this stage, compared to those in disadvantaged counties, people in advantaged counties may have more access to and resources to spend on social and recreational activities that boost mental health and social connections (
Astell-Burt and Feng 2021;
Larson et al. 2021;
Taff et al. 2021), draw on their savings to protect against the mental strain of job loss (
Despard et al. 2018), and leverage local social connections that may be more available in counties with good mental health (
Yang et al. 2019). In this stage, the health care infrastructure may be less burdened in counties with advantaged population health profiles (
Levin et al. 2023), potentially meaning there are more resources available for residents struggling with mental health and substance use problems and more hospital and emergency medical provider capacity to revive individuals who overdose. Inequalities start to wane in the third stage of the framework, as drug poisoning mortality starts to decline in disadvantaged counties toward the level of advantaged counties. The decline may reflect diffusion of information about accessing telehealth for substance use treatment (
Jones et al. 2022), the widespread distribution of government economic supports (
Wolf et al. 2024), the repeal of stay-at-home orders, bans on evictions and foreclosures to protect economically distressed households, and more. In the final stage, drug poisoning mortality rates approach similarly low levels in both types of counties.
Aims
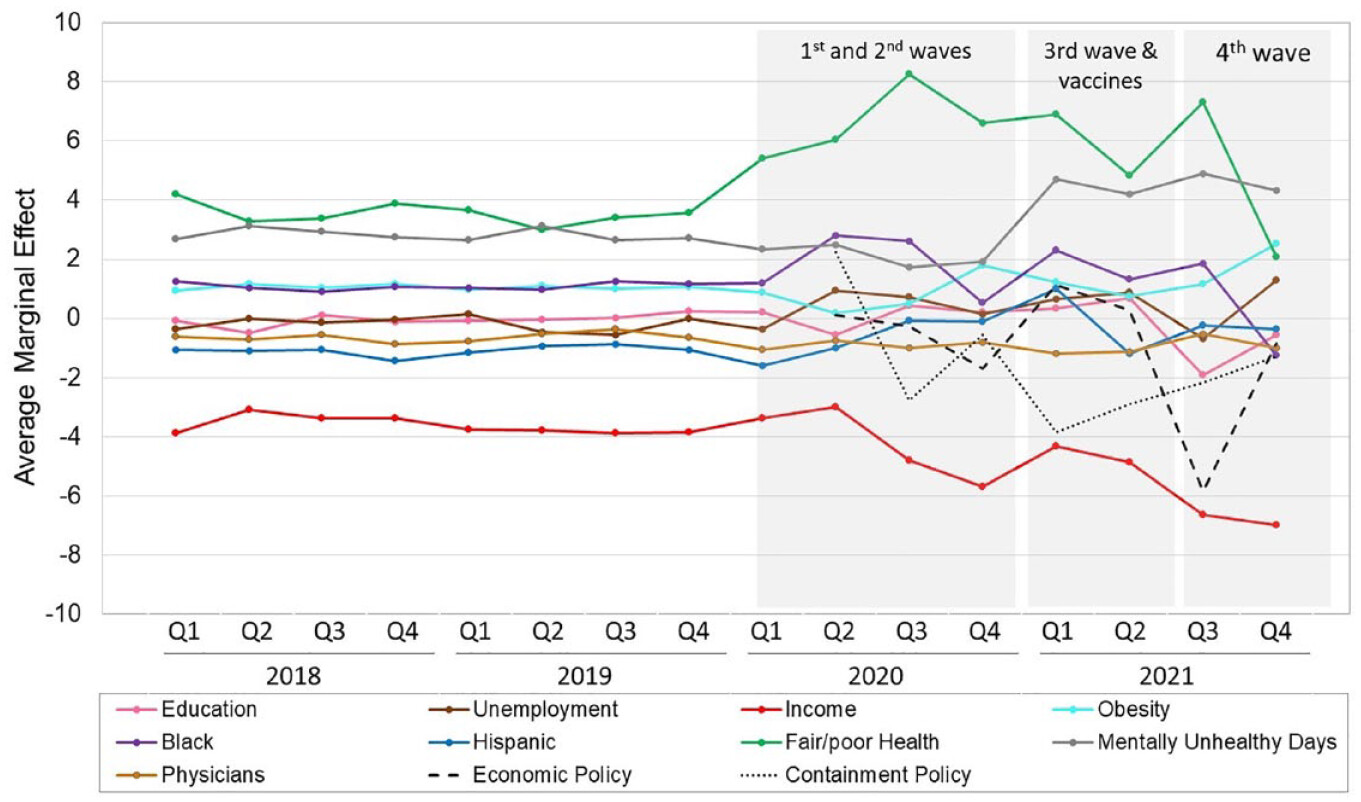
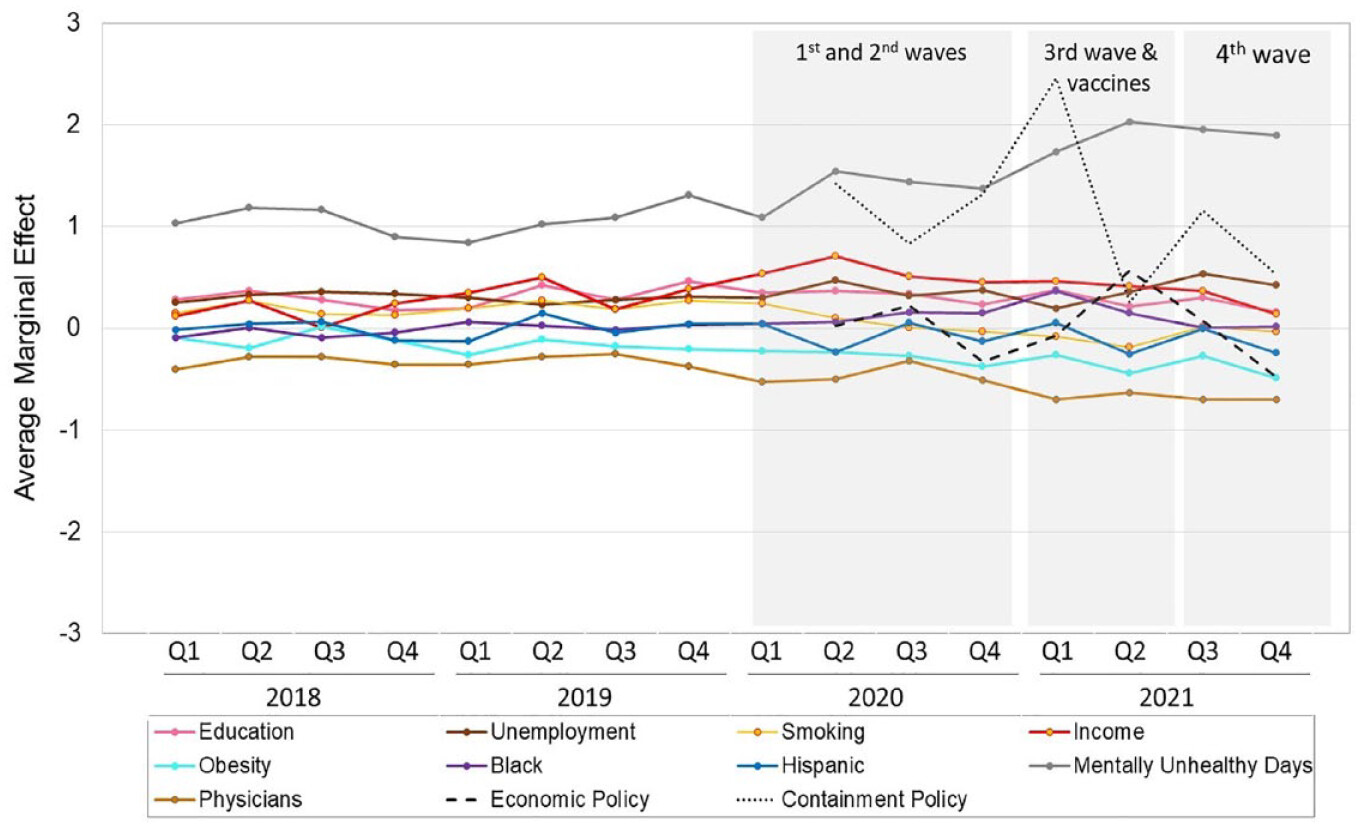
This study aims to better understand the contextual predictors of working-age mortality during the first two years of the COVID-19 pandemic in the United States and determine how they compare to the prepandemic period. The study uses county-level data to assess (1) how the importance of prepandemic county contexts for predicting deaths from all causes, drug poisoning, and COVID-19-related causes among working-age adults fluctuated during the pandemic; (2) how the importance of county contexts prior to and during the pandemic differed; and (3) their importance compared to states’ pandemic policies. We examine four domains of prepandemic county contexts: socioeconomic conditions, racial-ethnic composition, population health profile, and physician supply. The selection of these contexts was informed by the studies highlighted previously and the county health rankings and roadmap conceptual model for understanding all-cause mortality (
Remington, Catlin, and Gennuso 2015). We focus on counties because they are the smallest geographic unit for which mortality rates are available for the entire United States.
We focus on working-age adults (ages 25–64), whose mortality has been rising in recent decades (
National Academies of Sciences, Engineering, and Medicine [NASEM] 2021). We focus on them because (1) higher U.S. death rates vis-à-vis other high-income countries in 2020 and 2021 were most pronounced for adults under 65 years (
Bor et al. 2023), (2) U.S. life expectancy declines in 2020 and 2021 disproportionately involved COVID-19 deaths in midlife (
Masters, Aron, and Woolf 2024), and (3) although older adults had the highest COVID-19 mortality rates, working-age adults experienced the largest percentage increase in all-cause mortality over our study period.
1 Moreover, apart from COVID-19, unintentional injuries, driven by drug poisonings, was the cause of death that increased most during the pandemic (
Arias and Xu 2022), and drug poisoning mortality is highest among working-age adults (
Monnat 2023).
We extend prior work on how social inequalities in death fluctuated during the pandemic in several ways. First, rather than analyzing only COVID-19 deaths, we also consider drug poisoning and all-cause mortality because the pandemic’s impact was much broader than any single cause of death. Second, we include the prepandemic period, starting in 2018, to provide perspective on how much fluctuation was typical in the years preceding the pandemic. In addition, we account for states’ pandemic policies. The findings provide novel insights into how the exogenous shock of the pandemic disrupted the importance of contextual predictors of mortality.